


Abstract
Electrocardiographically (ECG) gated myocardial SPECT with 99mTc-tetrofosmin has been used widely to assess left ventricular (LV) function. However, the accuracy of variables using ECG gated myocardial SPECT with β-methyl-p-123I-iodophenylpentadecanoic acid (BMIPP) has not been well defined. Methods: Thirty-six patients (29 men, 7 women; mean age, 61.6 ± 15.6 y) with ischemic heart disease underwent ECG gated myocardial SPECT with 123I-BMIPP and with 99mTc-tetrofosmin and left ventriculography (LVG) within 1 wk. LV ejection fraction (LVEF), LV end-diastolic volume (LVEDV), and LV end-systolic volume (LVESV) were determined on gated SPECT using commercially available software for automatic data analysis. These volume-related items on LVG were calculated with an area–length method and were estimated by 2 independent observers to evaluate interobserver validity. The regional wall motion with these methods was assessed visually. Results: LVEF was 41.1% ± 12.5% on gated SPECT with 123I-BMIPP, 44.5% ± 13.1% on gated SPECT with 99mTc-tetrofosmin, and 46.0% ± 12.7% on LVG. Global LV function and regional wall motion between both gated SPECT procedures had excellent correlation (LVEF, r = 0.943; LVEDV, r = 0.934; LVESV, r = 0.952; regional wall motion, κ = 0.92). However, the correlations of global LV function and regional wall motion between each gated SPECT and LVG were significantly lower. Gated SPECT with 123I-BMIPP showed the same interobserver validity as gated SPECT with 99mTc-tetrofosmin. Conclusion: Gated SPECT with 123I-BMIPP provides high accuracy with regard to LV function and is sufficiently applicable for use in clinical SPECT. This technique can simultaneously reveal myocardial fatty acid metabolism and LV function, which may be useful to evaluate various cardiac diseases.
- gated SPECT
- β-methyl-p-123I-iodophenylpentadecanoic acid
- 99mTc-tetrofosmin
- left ventriculography
- left ventricular function
It is well established that left ventricular (LV) ejection fraction (LVEF) is an important tool in diagnostic and prognostic evaluation of patients with ischemic heart disease (1,2). A method of automatic quantification on electrocardiographically (ECG) gated myocardial SPECT developed by Germano et al. (3) clarified the accuracy of LVEF in comparison with first-pass radionuclide angiocardiography. Cardiac volume has also been confirmed by gated SPECT (4–7) because LVEF is obtained from the LV end-diastolic volume (LVEDV) and the LV end-systolic volume (LVESV): LVEF (%) = 100 × (LVEDV − LVESV)/LVEDV. These variables were first calculated using gated SPECT with 99mTc-sestamibi or 99mTc-tetrofosmin because they offered the advantage of a higher photon energy and higher injectable dose than 201Tl. Some recent studies have shown that gated SPECT with 201Tl has good correlation with radionuclide angiocardiography and contrast left ventriculography (LVG) with regard to LVEF and cardiac volume at rest (7–9). However, the possible use of gated SPECT with β-methyl-p-123I-iodophenylpentadecanoic acid (BMIPP) is unclear, although it has good accumulation and higher photon energy than 201Tl.
The objectives of this study were to assess the accuracy of variables on LV function, such as LVEF, LVEDV, and LVESV, using gated SPECT with 123I-BMIPP. Each variable using 123I-BMIPP was compared with each variable obtained from gated SPECT with 99mTc-tetrofosmin and from LVG.
MATERIALS AND METHODS
Study Population
Thirty-six patients (29 men, 7 women; age range, 40–82 y; mean age, 61.6 ± 15.6 y) underwent rest gated SPECT with 123I-BMIPP (Nihon Mediphysics, Nishinomiya, Japan) and 99mTc-tetrofosmin as well as LVG at rest within 1 wk to investigate ischemic heart disease. Eight patients were diagnosed with angina pectoris and 28 patients were documented as having myocardial infarction 1–8 mo before the study. Previous infarctions were located in the anterior myocardium (n = 18), the inferior myocardium (n = 7), and the lateral myocardium (n = 3). Seven patients had congestive heart failure. There were no patients whose condition changed remarkably between the examinations.
Gated SPECT Acquisition
Gated SPECT was performed at rest, 30 min after intravenous injection of 111–148 MBq 123I-BMIPP or 30–60 min after intravenous injection of 550–740 MBq 99mTc-tetrofosmin. SPECT acquisition was obtained with a dual-head gamma camera (Vertex; ADAC Laboratories, Milpitas, CA) equipped with low-energy, high-resolution collimators. Two heads were placed in an L-shaped configuration. Sixty-four projections (32 per head) from the 45° right anterior oblique position to the 45° left posterior oblique position were obtained as 64 × 64 matrices. Images were acquired for 50 s per projection on 123I-BMIPP or for 40 s per projection on 99mTc-tetrofosmin. The camera’s energy discriminator was set at the 159-keV photopeak of 123I with a 20% window or at the 140-keV photopeak of 99mTc with a 20% window. Imaging was gated at 8 frames per cardiac cycle using an R-wave trigger and acceptance window at 20% of the mean R-wave interval.
Gated SPECT Data Processing
The projection datasets were reconstructed with commercially available software (Cedars autoSPECT; ADAC Laboratories) on a Sun SPARC 20 workstation (Sun Microsystem Inc., Palo Alto, CA). Filtered backprojection with a Butterworth filter (order, 10.0; cutoff, 0.45 cycle/pixel on gated images; cutoff, 0.50 cycle/pixel on summed images) was performed. Attenuation was not corrected. The commercially available software that was used has been described (3). This program estimated the endocardial and epicardial surfaces for each interval and calculated the LVEF, LVEDV, and LVESV. The 8 intervals at each projection angle were compacted into 1 to reconstruct the summed image.
LVG
LVG images were acquired at 30 frames per second in a right anterior oblique 30° projection during injection of noniodinated contrast agent (Iopamiron; Schering Co., Berlin, Germany) through a 6-French pigtail catheter using the digital cardiac imaging system (CAS-10A; Toshiba Medical Co., Tokyo, Japan). The outlines of endocardial walls were drawn carefully with manual manipulation at end diastole and end systole. LV volumes and LVEF were calculated from single-plane cineangiograms by means of the area–length formula (10).
Image Analysis
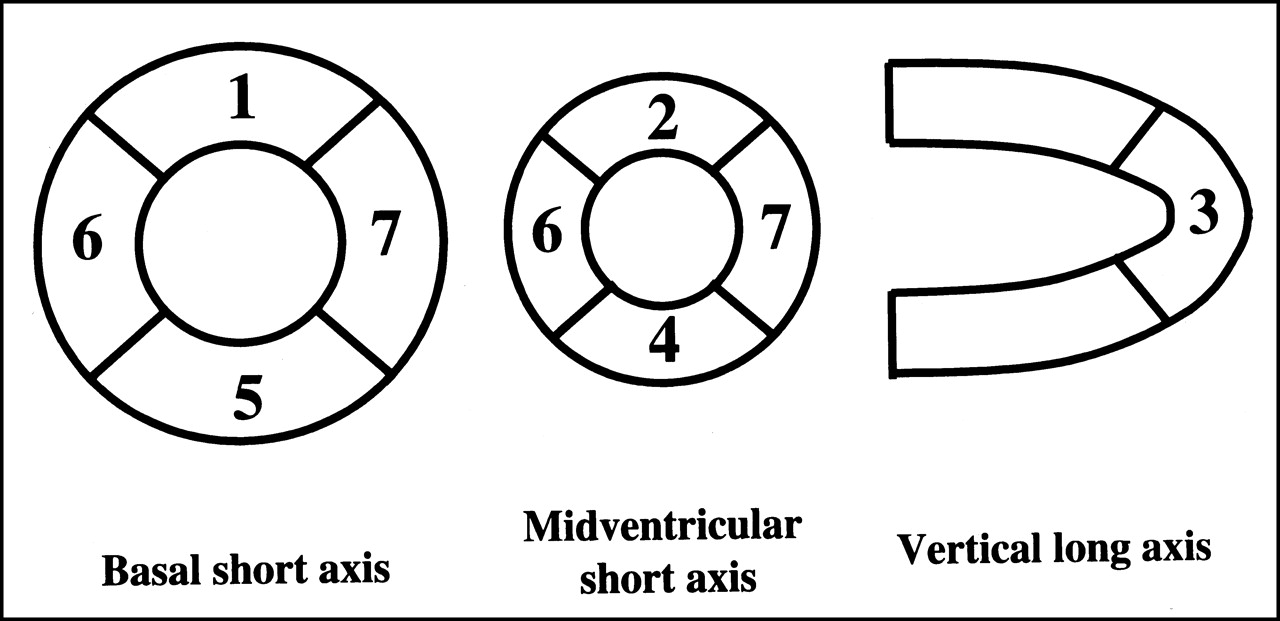
LV myocardium on both SPECT procedures and LVG was divided into 7 segments in compliance with the American Heart Association classification. The uptake of summed and gated SPECT was graded visually in all segments of each patient (Fig. 1) by the consensus of 2 observers who were unaware of the results of other tests. A 4-point scoring system was used to judge the quality of images (3 = excellent, 2 = good, 1 = fair, and 0 = poor) and to indicate the defect of segments (0 = normal, 1 = mildly reduced, 2 = severely reduced, and 3 = absent). The total defect score was defined as the summation of defect scores for each patient. The regional wall motion was scored visually on a 4-point scale using a smoothed cinematic display (0 = normal, 1 = mild hypokinesis, 2 = moderate to severe hypokinesis, and 3 = akinesis or dyskinesis).

Segmentation scheme used for regional assessment of defect scores and wall motion in SPECT.
Statistics
Categoric data were analyzed by the χ2 test. A paired t test was performed on continuous variables obtained form both gated SPECT procedures and LVG. The correlation (r) and linear regression between these data were calculated. The agreement among the 3 methods was assessed by Bland–Altman analysis (11). The agreement on regional functional measurements obtained from these analyses was evaluated from a 4 × 4 contingency table using κ statistics and the Spearman rank coefficient (12). Data are expressed as mean ± 1 SD. P < 0.05 is considered to be significant.
RESULTS
Myocardial SPECT Findings with 123I-BMIPP and 99mTc-Tetrofosmin
The total counts in a region of interest encompassing the myocardial area on projection images were 921 ± 214 kilocounts (kcts) on 123I-BMIPP and 1,221 ± 388 kcts on 99mTc-tetrofosmin (P < 0.01). The maximum and mean pixel counts on projection images of 123I-BMIPP and on projection images of 99mTc-tetrofosmin were 169 ± 24 counts (cts) and 241 ± 45 cts (P < 0.01) and 113 ± 13 cts and 161 ± 27 cts (P < 0.01), respectively. The total myocardial counts in all gated SPECT with 123I-BMIPP were lower than those with 99mTc-tetrofosmin (1,098 ± 222 kcts vs. 1,365 ± 563 kcts; P < 0.01). Gated SPECT with 123I-BMIPP had lower maximum and mean pixel counts than gated SPECT with 99mTc-tetrofosmin (maximum, 760 ± 83 kcts vs. 1,053 ± 188 kcts [P < 0.01]; mean, 253 ± 33 kcts vs. 393 ± 21 kcts [P < 0.01]), respectively. The quality of 3 summed images on 123I-BMIPP was excellent: 27 were good, 6 were fair, and 0 was poor. None of the gated images was excellent: 15 were good, 15 were fair, and 6 were poor. Among summed and gated images with 99mTc-tetrofosmin, 24 and 0 were excellent, 10 and 14 were good, 2 and 20 were fair, and 0 and 2 were poor, respectively. Summed images with 99mTc-tetrofosmin had significantly better quality (P < 0.01). No significant difference was found between both gated images. Total defect scores on summed SPECT with 123I-BMIPP and 99mTc-tetrofosmin were 6.2 ± 4.5 and 5.1 ± 3.9, respectively. Thirty-eight segments had no accumulation on summed SPECT with 123I-BMIPP and 28 segments had no accumulation on summed SPECT with 99mTc-tetrofosmin.
LV Function
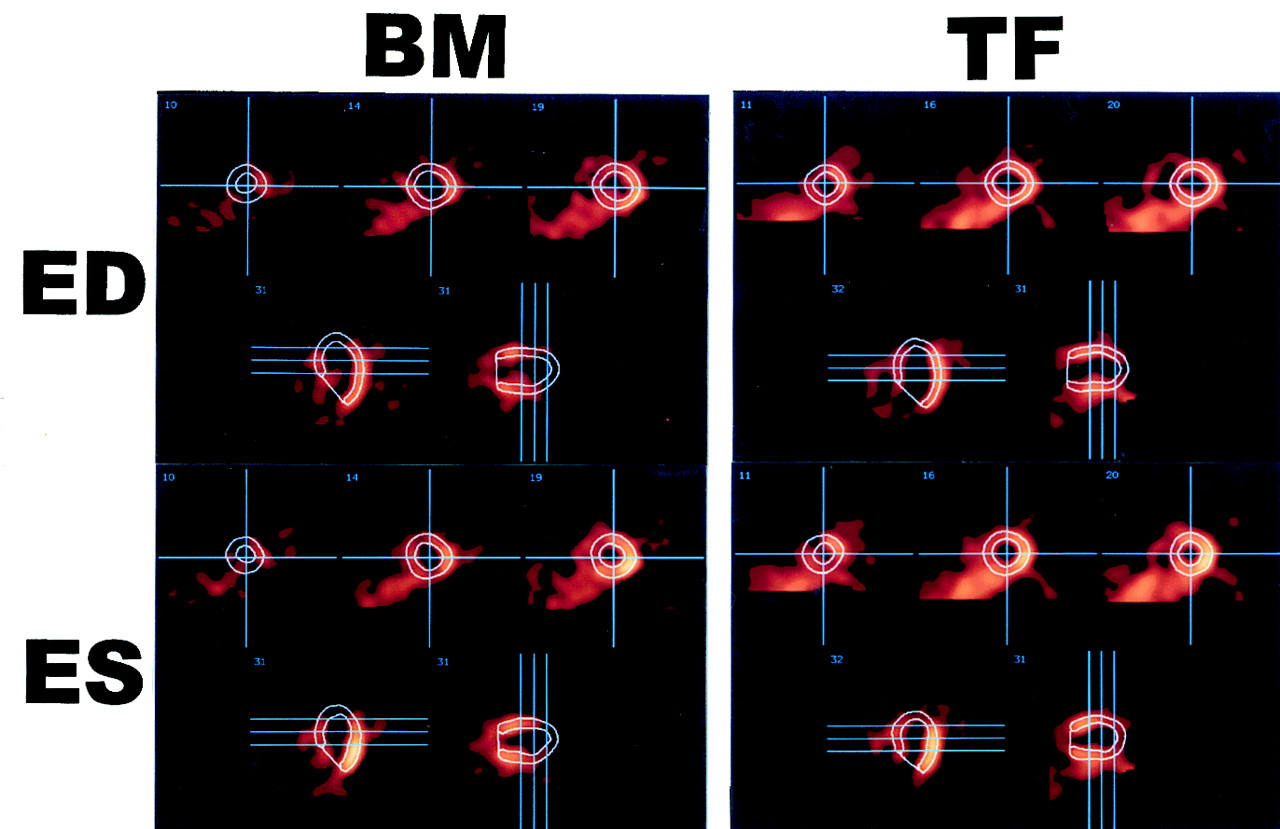
LVEF were calculated by automatically generating endocardial and epicardial contours (Fig. 2). Mean LVEFs were 41.1% ± 12.5% on gated SPECT with 123I-BMIPP, 44.5% ± 13.1% on gated SPECT with 99mTc-tetrofosmin, and 46.0% ± 12.7% on LVG. Mean LVEDV and LVESV were 113.2 ± 69.1 mL and 69.1 ± 39.1 mL, 118.1 ± 38.6 mL and 69.2 ± 35.2 mL, and 126.9 ± 35.1 mL and 69.5 ± 31.6 mL, respectively. No significant differences in the values were found between both gated SPECT procedures. LVEF and LVEDV obtained from gated SPECT with 123I-BMIPP were significantly lower than those of LVG (LVEF, P < 0.01; LVEDV, P < 0.01), and gated SPECT with 99mTc-tetrofosmin also had significantly lower LVEF and LVEDV (LVEF, P = 0.03; LVEDV, P = 0.02). LVESV did not show a significant difference between both gated SPECT procedures and LVG. No segment indicating dyskinesis and no LV aneurysm were observed by LVG.

End-diastolic (ED) and end-systolic (ES) images obtained from gated SPECT with 123I-BMIPP (BM) and 99mTc-tetrofosmin (TF) in patient with anterior myocardial infarction.
Relation Between Gated SPECT with 123I-BMIPP and with 99mTc-Tetrofosmin
Linear regression analyses of LVEF, LVEDV, and LVESV between gated SPECT with 123I-BMIPP and 99mTc-tetrofosmin are shown in Figure 3. The results correlated well with r = 0.943 for LVEF, 0.934 for LVEDV, and 0.952 for LVESV. The Bland–Altman analyses were also shown in Figure 3. Mean differences of 3.9% ± 5.5% for LVEF, 4.8 ± 13.3 mL for LVEDV, and 0.1 ± 9.8 mL for LVESV were observed. No significant degree of systematic measurement bias on LVEF and LVESV was found between the 2 isotopes. However, a significant, but small, negative linear regression of 0.37 with an intercept at 20.82 mL was indicated on the Bland–Altman trend for LVEDV. This slope showed that 173.5 mL was the same LVEDV value obtained from both gated SPECT procedures. Linear regression analysis of LVEF, LVEDV, and LVESV between the total defect score of summed SPECT with 123I-BMIPP and the differences between both gated SPECT procedures are shown in Figure 4. No significant correlations were found between them. Table 1 shows the relationship of regional wall motion scores between both gated myocardial SPECT procedures (exact agreement, 94.0%; κ, 0.89). On gated SPECT with 123I-BMIPP, 98.4% of the regional wall motion scores were within 1 point of the corresponding gated SPECT with 99mTc-tetrofosmin.
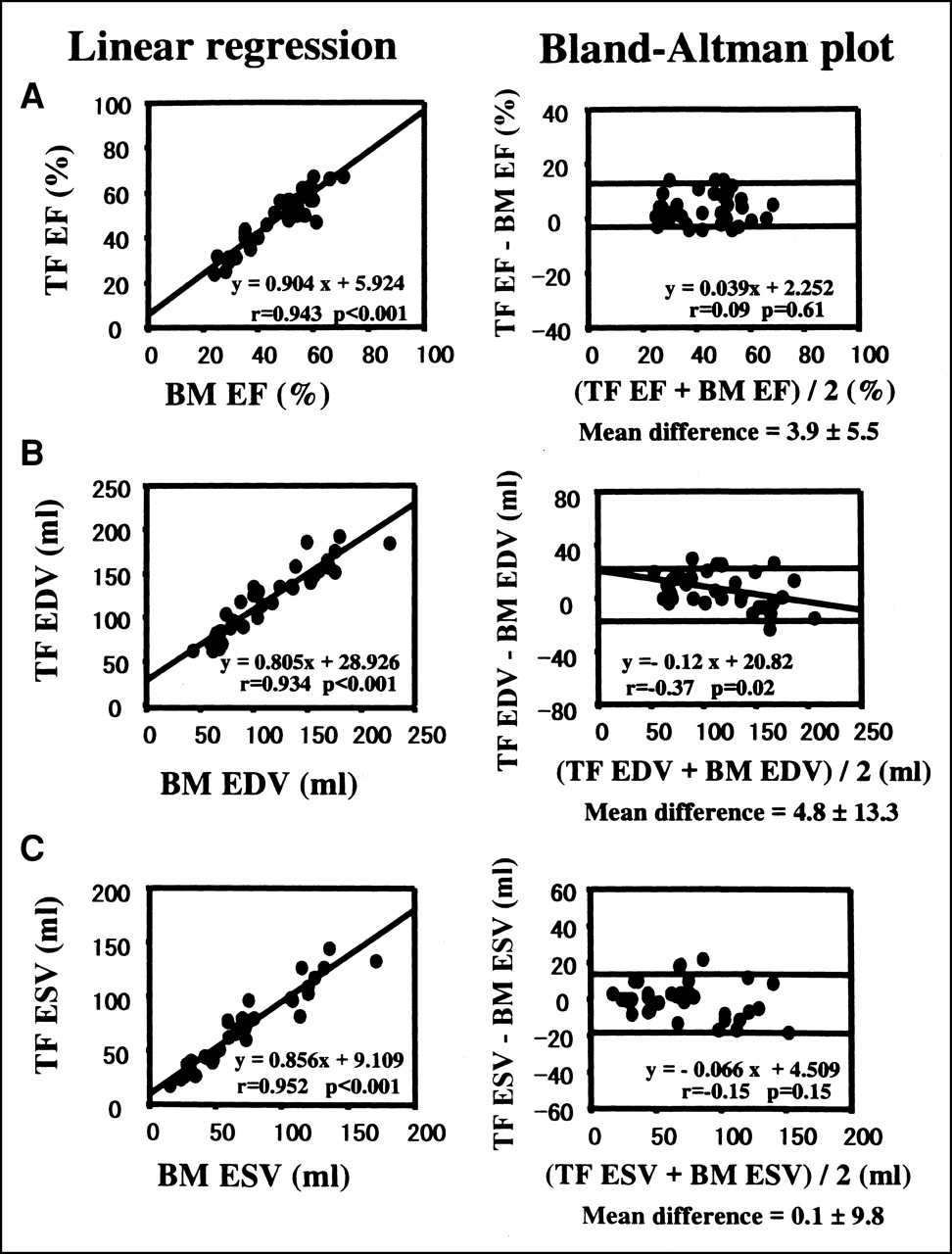
Comparison of LVEF (EF), LVEDV (EDV), and LVESV (ESV) obtained from gated SPECT with 123I-BMIPP (BM) and 99mTc-tetrofosmin (TF).

(Left) Linear regression analysis of total defect score (TDS) of gated SPECT with 123I-BMIPP (BM) and differences between both gated SPECT procedures on LVEF (EF), LVEDV (EDV), and LVESV (ESV). TF = 99mTc-tetrofosmin. (Right) Linear regression analysis of TDS of gated SPECT with 123I-BMIPP and differences between gated SPECT with 123I-BMIPP and LVG on EF, EDV, and ESV.
Agreement Between 123I-BMIPP and 99mTc-Tetrofosmin Gated SPECT Segmental Wall Motion Scores
Relation Between Both Gated SPECT Procedures and LVG
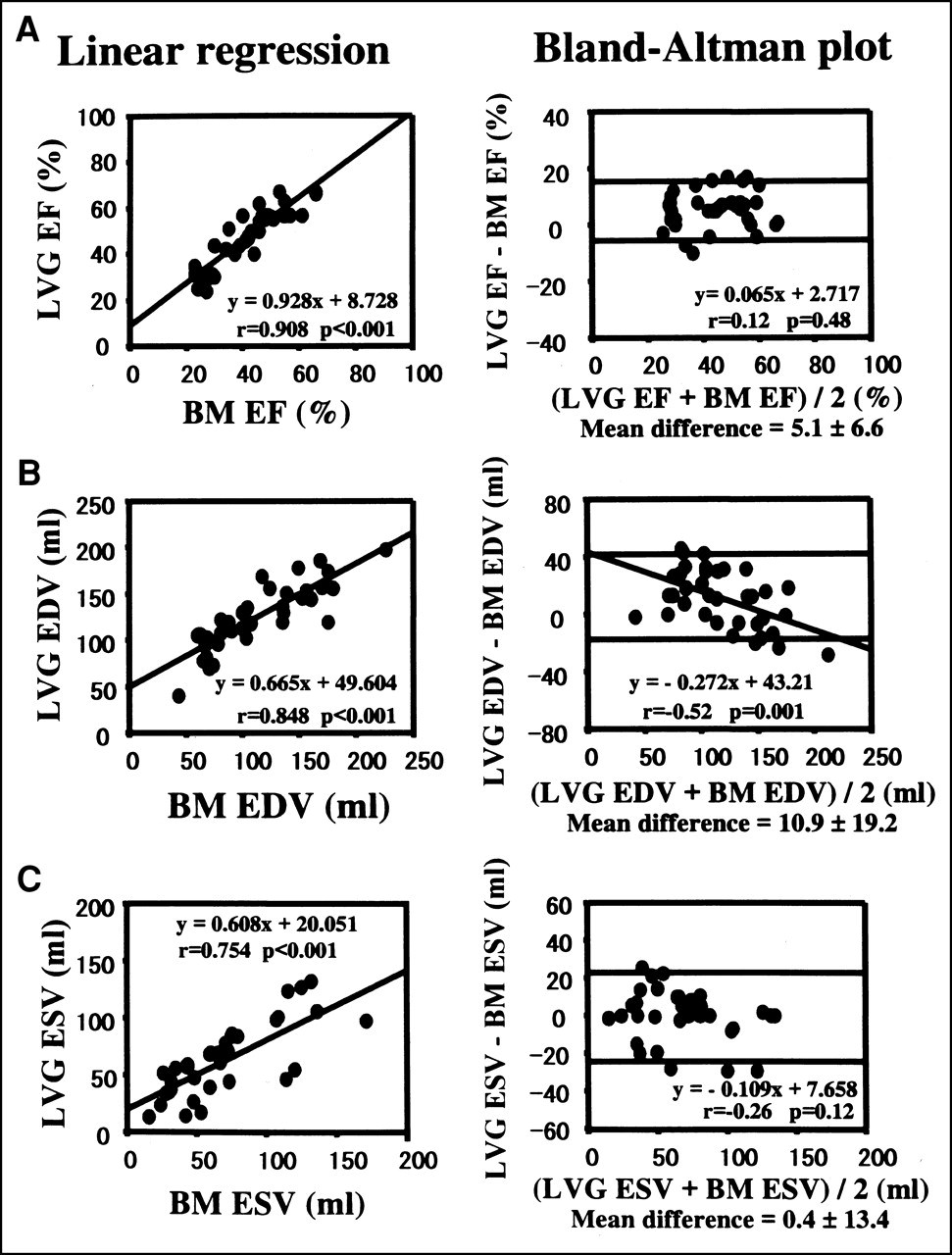
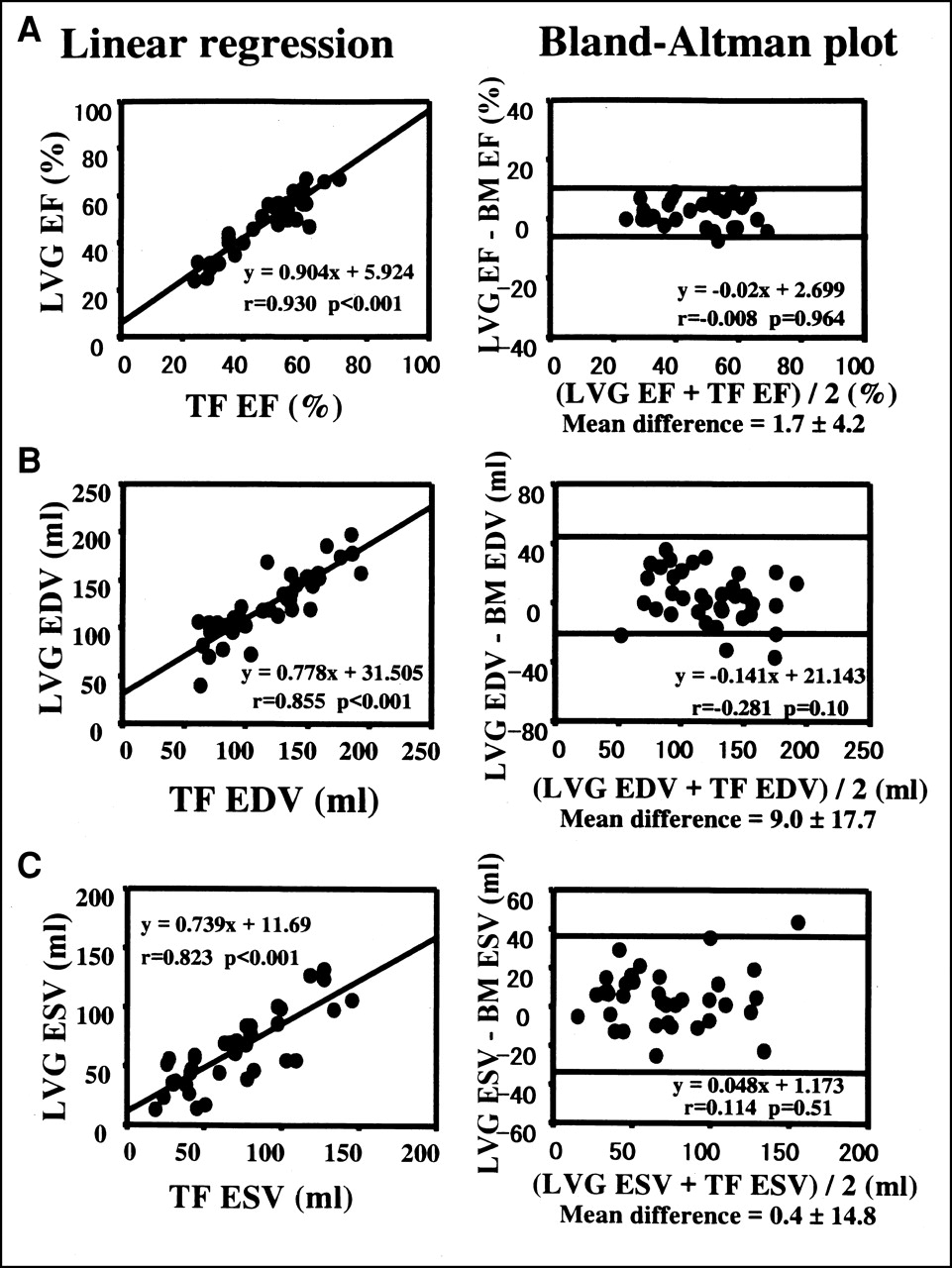
Linear regression analyses of LVEF, LVEDV, and LVESV between gated SPECT with 123I-BMIPP and LVG are shown in Figure 5. The results of them correlated well with r = 0.908 for LVEF, 0.848 for LVEDV, and 0.754 for LVESV. Although the correlation coefficients were significant, they were lower than those between both gated SPECT procedures. The Bland–Altman analyses between gated SPECT with 123I-BMIPP and LVG are shown in Figure 5. Mean differences of 6.1% ± 6.6% for LVEF, 10.9 ± 19.2 mL for LVEDV, and 0.4 ± 3.4 mL for LVESV were observed. No significant degree of systematic measurement bias on LVEF and LVESV was found between the gated SPECT with 123I-BMIPP and LVG. However, a significant, but small, negative linear regression of 0.52 with an intercept at 43.21 mL was indicated on the Bland–Altman trend for LVEDV. This slope showed that 158.8 mL was the same LVEDV value obtained from gated SPECT with 123I-BMIPP and LVG. Linear regression analyses of LVEF, LVEDV, and LVESV between total defect score of summed SPECT with 123I-BMIPP and differences between gated SPECT with 123I-BMIPP and LVG are shown in Figure 4. No significant correlations were found between them. On the other hand, gated SPECT with 99mTc-tetrofosmin had good correlations with LVG with r = 0.930 for LVEF, 0.855 for LVEDV, and 0.823 for LVESV, respectively (Fig. 6). The Bland–Altman analysis showed no significant degree of systematic measurement bias on these values between gated SPECT with 99mTc-tetrofosmin and LVG (Fig. 6).
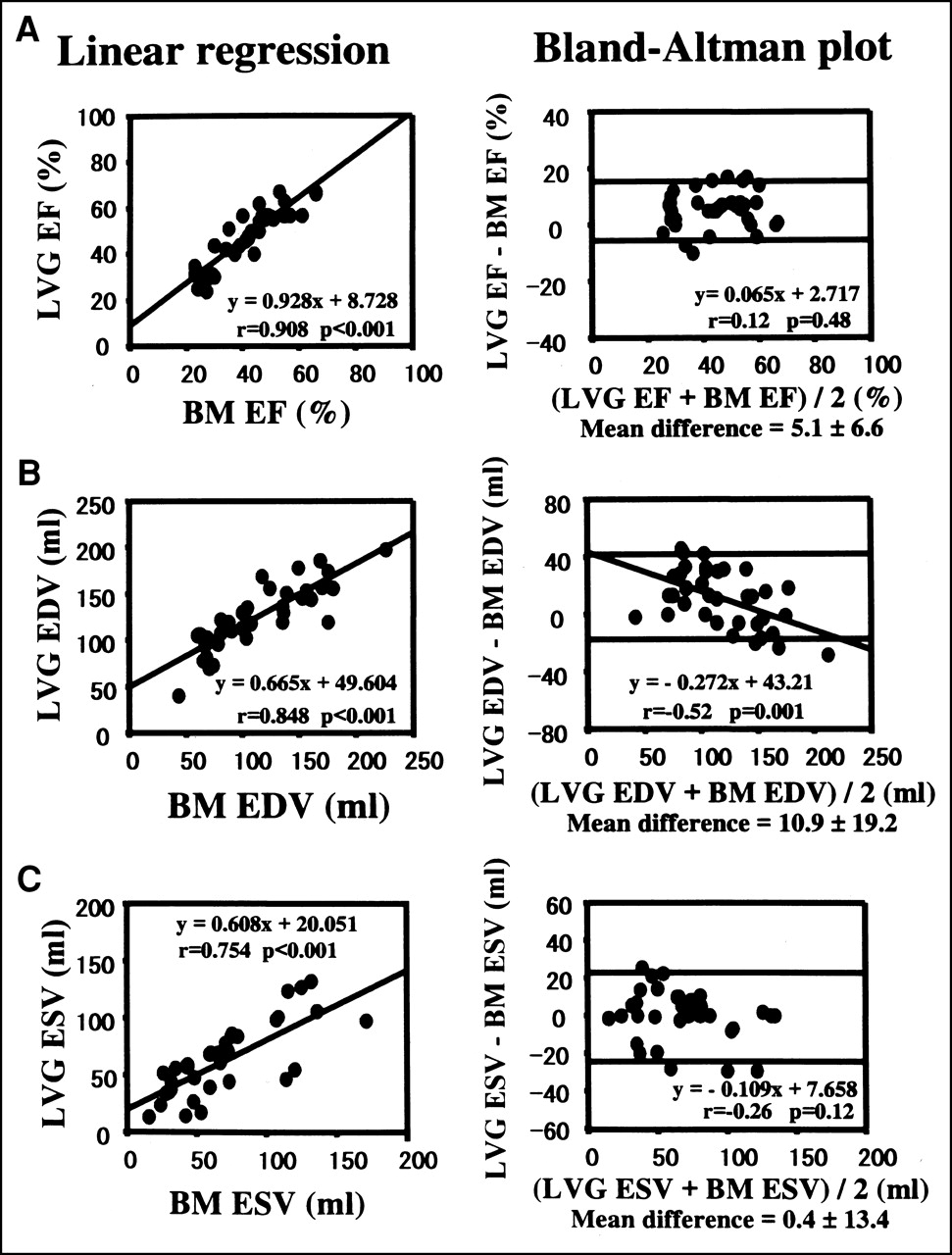
Comparison of LVEF (EF), LVEDV (EDV), and LVESV (ESV) obtained from gated SPECT with 123I-BMIPP (BM) and LVG.

Comparison of LVEF (EF), LVEDV (EDV), and LVESV (ESV) obtained from gated SPECT with 99mTc-tetrofosmin (TF) and LVG.
For the assessment of regional wall motion, the comparisons between gated SPECT with 123I-BMIPP and LVG and between gated SPECT with 99mTc tetrofosmin and LVG yielded an exact agreement of 89.2% (κ = 0.81; Table 2) and 83.3% (κ = 0.72; Table 3) on wall motion score, respectively. In comparison, Table 2 shows that 96.8% of the wall motion scores of gated SPECT with 123I-BMIPP were within 1 point of the corresponding LVG. Table 3 shows that 94.8% of the wall motion scores of gated SPECT with 99mTc-tetrofosmin were within 1 point of the corresponding LVG.
Agreement Between 123I-BMIPP Gated SPECT and LVG Segmental Wall Motion Scores
Agreement Between 99mTc-Tetrofosmin Gated SPECT and LVG Segmental Wall Motion Scores
Interobserver Validation of Gated SPECT with 123I-BMIPP
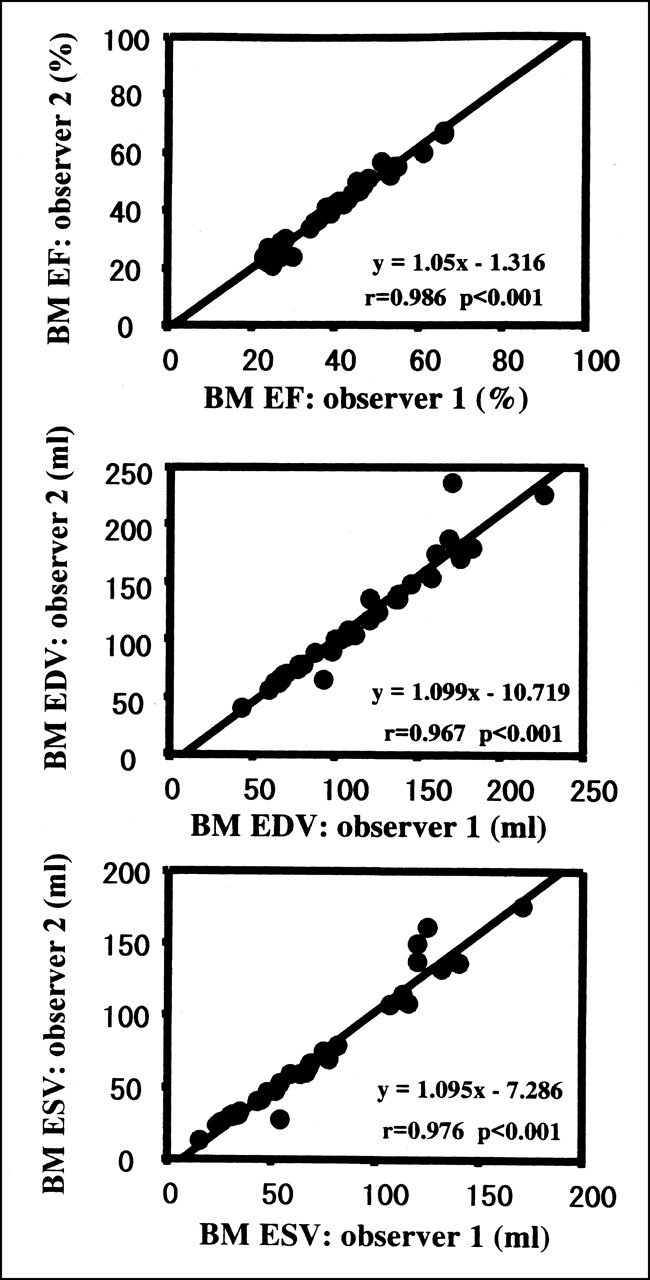
The reliability of interobserver validation was verified on LVEF and LV volumes from both gated SPECT procedures and LVG. The LVEF and LV volumes obtained from gated SPECT with 123I-BMIPP showed a good correlation between 2 independent observers (Fig. 7). Those obtained from gated SPECT with 99mTc-tetrofosmin also showed a good correlation between the 2 analyses. Correlation coefficients were 0.996 on LVEF, 0.996 on LVEDV, and 0.996 on LVESV, respectively. Those obtained from LVG on the first analysis had a significant, but weaker, correlation with the second analysis on LVEF (r = 0.81), LVEDV (r = 0.79), and LVESV (r = 0.75), respectively.

Linear regression analysis of LVEF (EF), LVEDV (EDV), and LVESV (ESV) on gated SPECT with 123I-BMIPP (BM) measured by 2 independent observers.
DISCUSSION
Several modalities have been developed to calculate LVEF and LV volumes accurately because these parameters greatly affect the management of patients with ischemic heart disease (1,2). One of the earliest methods to measure LVEF and LV volumes is constrast LVG. However, this method has a potential for error in measuring LV volumes because it assumes that the left ventricle can be represented by a 3-dimensional ellipsoid reference figure. Moreover, this method is so invasive that it could cause complications in patients who undergo it. Automatic quantification on gated SPECT has been used widely in clinical SPECT studies to evaluate LV function. This technique measures LV volumes in 3-dimensional space and offers not only LV function but also functional myocardial imaging. Nevertheless, there has been little experience in applying this technique to gated SPECT, with the exception of perfusion tracers.
Inubushi et al. (13) reported application of 123I-BMIPP to gated SPECT and showed that gated SPECT with 123I-BMIPP had a good correlation with gated SPECT using 99mTc-sestamibi on LVEF, even in patients with a large defect. In this study, LVEF, LV volumes, and regional wall motion obtained from gated SPECT with 123I-BMIPP correlated well with those from gated SPECT with 99mTc-tetrofosmin. This study revealed that the total defect score did not influence the differences on LVEF and LV volumes between gated SPECT with 123I-BMIPP and the other modalities. The results were quite consistent with those in an earlier report (13). Because LVEF was calculated by dividing the difference between LVEDV and LVESV by LVEDV, some patients have similar values of LVEF, even if the values of LVEDV and LVESV are quite different. The current study verified that absolute LV volumes calculated with gated SPECT with 123I-BMIPP were similar to those with 99mTc-tetrofosmin. This finding confirms that LVEF obtained from gated SPECT with 123I-BMIPP is more accurate. Accurate measurements of LV volume are also clinically useful because LVEDV and LVESV themselves influence the prognosis in patients with ischemic heart disease (14,15).
A significant, but small, negative linear regression was indicated on the Bland–Altman trend for LVEDV. This result might mean that gated SPECT with 123I-BMIPP potentially underestimates LVEDV in patients with small LV cavity size and overestimates LVEDV in patients with a dilated LV cavity. This underestimation does not matter in clinical use because it is well known that this software inaccurately calculates LV volumes in patients with small LV cavity size and it is not used for such patients. Gated SPECT with 123I-BMIPP is clinically applicable except for patients with severely dilated heart, considering that the LVEDV of both gated SPECT procedures was the same (173.5 mL) and that the mean LVEDV of gated SPECT with 123I-BMIPP was lower.
Data on the regional wall motion obtained from both gated SPECT procedures showed good correlation and agreement. This result was consistent with the findings of earlier studies (16–18). Gated SPECT with 99mTc-tetrofosmin provides an accurate assessment of regional wall motion in comparison with other modalities such as MRI (16,17) and sonographic cardiography (18). Therefore, gated SPECT with 123I-BMIPP has significant reliability to assess regional wall motion. In addition, gated SPECT with 123I-BMIPP provided excellent interobserver reproducibility. These results suggest that gated SPECT with 123I-BMIPP is applicable in the same manner as gated SPECT with 99mTc-tetrofosmin.
LV volumes of LVG have been compared with those of gated SPECT with perfusion tracers (4,19,20). Yoshioka et al. (4) also showed that LVEF and LVEDV obtained from gated SPECT were significantly lower than those from LVG. Nichols et al. (19) reported similar results and suggested that inclusion of a greater portion of the outflow tract caused additional angiographic volume. It is widely acknowledged that LVG potentially overestimates the true volume for various reasons, such as the fact that contrast material fills intramyocardial interstices and that the increase in preload by the infusion of contrast material results in hypercontractility of the LV wall. One report indicates that LV volumes calculated from single-plane cineangiograms by means of the area–length method overestimate true LV volumes determined by postmortem LV cast (10). In the current study, LVEF and LVEDV of gated SPECT with 123I-BMIPP were lower than those of LVG. Because gated SPECT with 123I-BMIPP correlated well with LVG on LVEF and LV volumes and because the Bland–Altman analysis between gated SPECT with 123I-BMIPP and LVG showed results similar to those of earlier reports (4,7) using 99mTc-tetrofosmin or 99mTc-sestamibi, the results of this study are reasonable, considering these background factors. In the same manner as the Bland–Altman plot between both gated SPECT procedures, a significant, but small, negative linear regression was indicated on the Bland–Altman trend for LVEDV between gated SPECT with 123I-BMIPP and LVG. However, this result has little influence on clinical use.
The assessment of regional wall motion plays an important role in the diagnosis and severity of ischemic heart disease. These data showed excellent agreement in the regional wall motion between gated SPECT with 123I-BMIPP and LVG. William and Taillon (20) showed that regional wall motion from gated SPECT with perfusion tracer correlated well with that from LVG. Gated SPECT with 123I-BMIPP could be transposed from LVG in the evaluation of regional wall motion.
Finally, gated SPECT with 123I-BMIPP had sufficient myocardial counts on 8-gated images in this study. Gated SPECT with 99mTc-tetrofosmin or 99mTc-sestamibi has been developed on 8-gated images. This method has been applied to 16-gated images to obtain a more accurate LVEF. This method requires a higher count density in comparison with 8-gated images. Gated SPECT with a lower count density is assumed to cause overestimation of LVEDV (8), and the Bland–Altman trend indicated the possibility of overestimation of LVEDV in patients with dilated hearts. The current study revealed that SPECT with 123I-BMIPP had sufficient myocardial counts on 8-gated images. Because the myocardial counts on gated SPECT with 123I-BMIPP were three fourths of those on gated SPECT with 99mTc-tetrofosmin, one might be able to apply SPECT with 123I-BMIPP to 16-gated images, hoping to obtain a higher count density.
Clinical Implication
Myocardial SPECT supplies physiologic information on the myocardium in vivo through imaging. Images obtained from radionuclide tracers in clinical use should indicate true information such as myocardial perfusion and free fatty utilization in the myocardium. However, differences are sometimes found between the results of myocardial SPECT and other modalities because artifacts are generated in the process from acquisition to reconstruction of imaging. Various corrections, such as attenuation correction and scattered correction, have been developed to obtain more accurate results. On the basis of earlier studies (21–23), supplementing the regional wall motion in functional imaging increases the accuracy of diagnosis of cardiac diseases, resulting from exclusion of artifacts by attenuation or regional wall motion. Moreover, Choi et al. (21) reported that gated SPECT provided improved differential accuracy in the equivocal reduced uptake area, which often puzzled observers. This technique could provide additional information to diagnose more exactly various heart diseases.
Previous reports have indicated that 123I-BMIPP is taken into the triglyceride pool and reflects fatty acid utilization in the myocardium (24,25). Clinical studies using 123I-BMIPP have shown the efficacy in the diagnosis and the assessment of severity on ischemic heart diseases such as vasospastic angina (26) and unstable angina (27). Hashimoto et al. (28) reported that a discordance between the perfusion tracer and 123I-BMIPP after myocardial infarction predicted subsequent improvement of LV contractility. In other studies, the degree of regional uptake of 123I-BMIPP in patients after myocardial infarction correlated well with regional wall motion (29,30) and predicted future cardiac events in combination with myocardial perfusion tracer (31,32). This imaging might be of use in the evaluation of patients after myocardial infarction.
There is no doubt that LVEF is an important variable in the management of patients with ischemic heart disease. However, LV remodeling also has a huge impact on the prognosis of patients with ischemic heart disease. Lee et al. (14) reported that LV volume was an independent predictor of cardiac events in patients with severe congestive heart failure. Kjøller-Hansen et al. (15) have shown recently that increases in LVEDV index and LVESV index predicted an increasing risk of a future adverse cardiac outcome, even in patients without clinical heart failure. Accurate measurement of not only LVEF but also LV volumes is beneficial in the management of patients with ischemic heart disease. Moreover, LV function and the size of the myocardial infarction play important roles in LV remodeling after myocardial infarction. Because this technique simultaneously evaluates both parameters, LV remodeling after myocardial infarction might be predicted more precisely.
It is well known that regional uptake of 123I-BMIPP is reduced in the septum of patients with hypertrophic cardiomyopathy (33,34). Sugihara et al. (35) reported that patients with complete left bundle branch block have reduced uptake of 123I-BMIPP in the septum. This reduced uptake of tracer is assumed to be associated with the abnormality of the regional contraction. However, gated SPECT with 123I-BMIPP might offer suggestions as to the more detailed mechanism and the relationship between the reduced uptake of 123I-BMIPP and the regional wall motion because this technique concurrently estimates the regional wall motion and regional uptake.
Potential Study Limitations
In this study, we applied gated SPECT with 123I-BMIPP to commercially available software and showed that this technique was acceptable to measure LV function clinically. Previous reports showed that 99mTc-tetrofosmin had a 1.2% accumulation rate and an energy peak at 140 keV (36) and that 123I-BMIPP had a 4.8% accumulation rate and an energy peak at 159 keV (37). On the other hand, 201Tl has a 3.9% accumulation rate and an energy peak from 70 to 80 keV (38). Because the count density of 123I in this study was sufficient to obtain accurate LVEF and LV volumes (39), 123I-BMIPP has an adequate kinetic profile in vivo to be applied as a tracer on gated SPECT. However, to our knowledge, the effects of using gated SPECT with 123I-BMIPP (using a phantom model with 123I-BMIPP) on LVEF, LV volumes, and regional wall motion have not been investigated.
First, filtering and zooming influence the measurement of LVEF, LVEDV, and LVESV in gated SPECT with 201Tl (40). There is some possibility that the alteration of each parameter changes the results and makes the manipulation more complex. The use of gated SPECT with a lower cutoff frequency calculates lower LVEF, even in gated SPECT with 99mTc-sestamibi. On the contrary, a high cutoff frequency overestimates LVEDV and, consequently, overestimates LVEF (8) because the filter lowers the count density of the left myocardium. The high cutoff frequency used posed no problem for gated SPECT with 123I-BMIPP in this study population because gated SPECT with 123I-BMIPP did not calculate larger LV volumes. This, finding might relate to the filter setting; however, a significant, but small, negative linear regression was indicated on the Bland–Altman trend for LVEDV. Further investigation is necessary to verify the reliability of gated SPECT with 123I-BMIPP.
Second, only patients with ischemic heart disease were subjects in this study. Earlier investigation of gated SPECT with 123I-BMIPP showed that it correlated well with gated SPECT with 99mTc-tetrofosmin, even in patients with extensive reduced uptake in the left ventricle (15). However, it is well known that extensive reduced uptake of tracer in the left ventricle and LV hypertrophy influence LVEF and LV volumes calculated with gated SPECT. Thus, further investigation is needed to apply this technique to patients with hypertrophic cardiomyopathy, especially that with asymmetric hypertrophy.
CONCLUSION
Accurate LVEF and LV volumes were obtained with ECG gated myocardial SPECT with 123I-BMIPP. This image can simultaneously show myocardial fatty acid metabolism and LV function and, therefore, may be useful for investigating various cardiac diseases.
Acknowledgments
The authors thank Ichiro Nanbu, MD, Yoshimi Kinoshita, MD, Mitsuo Sugimoto, RT, and Ken-ichi Kamegai, RT, at the Nagoya Daini Red Cross Hospital for their technical assistance and interesting suggestions.
Footnotes
Received Mar. 5, 2001; revision accepted Aug. 20, 2001.
For correspondence or reprints contact: Mamoru Nanasato, MD, Cardiovascular Center, Nagoya Daini Red Cross Hospital, 2-9 Myouken-cho, Showa, Nagoya, 466-8650 Japan.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.