


Abstract
The aim of this study was to compare the accuracy of 99mTc-methoxyisobutylisonitrile scintimammography (SMM) and conventional mammography in patients presenting with suspected primary breast cancer. Receiver-operating-characteristic (ROC) curve analysis was applied to determine if a combination of x-ray mammography (XMM) and SMM was more accurate than a single test alone. Methods: The results of SMM, XMM, and a combination of both studies performed over a 3-y period on 374 suspicious lesions in 353 patients with no previous history of breast cancer were reviewed. Each scan report was reviewed and graded as follows: grade 1, definitely normal or benign; grade 2, probably normal or benign; grade 3, equivocal; grade 4, probably cancer; and grade 5, definitely cancer. The results were verified by pathologic examination of biopsy material obtained from each suspicious mass. ROC curves were generated from these results. Results: There were 204 malignant breast tumors and 170 nonmalignant breast lesions. SMM diagnosed correctly 181 breast cancers and was true-negative in 122 benign breast lesions: sensitivity, 89%; specificity, 71%; positive predictive value (PPV), 79%; and negative predictive value (NPV), 84%. XMM diagnosed correctly 143 malignant tumors and was true-negative in 117 nonmalignant lesions. The sensitivity, specificity, PPV, and NPV for XMM were 70%, 69%, 73%, and 66%, respectively. Using a combination of the two tests, the combined sensitivity was 93%, specificity was 72%, PPV was 80%, and NPV was 90%. Using the index of the area under the ROC curve obtained by the rating method showed that the combination of XMM and SMM was significantly more accurate than either of the individual tests if performed alone (P < 0.05). Conclusion: This study shows that the combination of XMM and SMM produces more accurate results than either modality alone. Therefore, if there is doubt about the accuracy of XMM, SMM should be used as the second-line test in breast imaging.
In most western countries breast cancer is the most common malignancy among women. England and Wales have the highest mortality rates in Europe, and this cancer accounts for about 27 deaths per 100,000 women per year (1,2). It is unclear if this increased mortality is associated with differences in the diagnosis and treatment of breast cancer in England and Wales or if it is associated with differences in the nature of the disease. What is known is that the mortality rate is dependent on the early accurate detection of breast cancers and subsequent treatment (3).
At present, the main methods used for the detection of malignant breast lesions have been mammography and physical examination performed by the patient or by a trained physician. Conventional x-ray mammography (XMM) is not ideal for determining the presence of cancer and may have a false-negative rate of 10%–20% (4,5). Interpretation of the mammogram is often more difficult in women with dense breasts, in the young patient, and in those who are on hormone replacement therapy (6); the positive predictive value (PPV) may be as low as 15%–39% for nonpalpable tumors and 22% for palpable tumors (4).
Functional imaging using a tumor-avid radiopharmaceutical may be useful in those cases in which anatomic imaging alone proves to be difficult. The best agent for imaging breast cancer appears to be 99mTc-methylisobutylisonitrile (MIBI). MIBI is a marker of cellular activity and has significant uptake in a range of tumors, including breast cancer (7–9). Scintimammography (SMM) has a sensitivity and specificity of 72%–100% for the diagnosis of breast cancer (10–14). It would appear that no single test is ideal, and a combination of anatomic imaging of the breast by mammography and functional imaging with SMM may be required to ensure that it is possible to find breast cancer, especially when mammography is at a disadvantage.
As the imaging community has become concerned with the measurement of the information content of various imaging modalities, receiver-operating-characteristic (ROC) curves have become increasingly popular (15–17). It is also the statistical method of choice for testing the accuracy of a combination of imaging methods (18).
The aim of this study was to compare the diagnostic accuracy of 99mTc-MIBI SMM and XMM alone and also used as a sequence of XMM followed by SMM in the diagnosis of primary breast cancer using ROC curve analysis.
MATERIALS AND METHODS
Patients
A retrospective review was performed of 353 consecutive female patients who were imaged with both methodologies for clinical reasons (and not for a specific research protocol) for suspected primary breast cancer over a 5-y period. Fifty-four patients were <40, 105 were 41–50, 98 were 51–60, and 96 were >60 y old. Patients were selected if there was concern over the result of mammography or disagreement between the results of mammography and physical examination of the breast and if they were having definitive core or surgical biopsy so that pathology could be verified. Patients were imaged before biopsy was performed. There were 374 lesions suggestive of breast cancer presenting as a palpable mass or abnormality in the breast or having been seen as a suspicious area on mammography. The mean age ± SD of the patients was 53 ± 12 y (range, 28–85 y). One hundred forty-seven patients were <50 y old (39%). The mean time interval between the two imaging modalities was 6 d (range, 1–28 d). Patients were imaged within 6 wk of definitive biopsy.
XMM
Patients with suspected breast cancer were imaged using standard two-view XMM, which was performed using a dedicated mammography unit (DMR; International General Electric, Paris, France). A standard two-view protocol of craniocaudal and lateral oblique views was used with 26- to 28-keV x-rays and automatic exposure control. The images were interpreted by a radiologist who was a trained specialist, with knowledge of the patient’s history, clinical presentation, and the results of previous mammograms, if available. Cancer was diagnosed when there was a spiculated or irregular dense lesion, suspicious microcalcifications, or other changes in breast tissue architecture compared with previous mammography. The clinical reports of all patients were reviewed and graded using a simple five-point grading system: grade 1, definitely normal or benign; grade 2, probably normal or benign; grade 3, equivocal; grade 4, probably cancer; and grade 5, definitely cancer.
SMM
Radionuclide imaging was performed 5–10 min after intravenous injection of 740 MBq 99mTc-MIBI (DuPont Pharma, Billerica, MA) in a foot vein. All patients were imaged using prone-dependent lateral and supine anterior planar imaging (5,15). This method was used to provide maximum separation of the breast from underlying thoracic activity. Planar images were obtained with a 256 × 256 matrix, imaging with 15% windows around a 140-keV photopeak and with an acquisition time of 10 min for both lateral and anterior views, using a two-head gamma camera (Prism 2000XP; Picker International, Cleveland Heights, OH). A high-resolution, low-energy collimator was used in each case. After obtaining the 10-min image of each breast, another image was obtained with 57Co markers placed on the nipple. The anterior view was obtained with the patient supine and both arms held above the head. Studies were reported by a specialist in nuclear medicine using the same five grades as were used in reporting of the XMM. All 99mTc-MIBI images were interpreted with the specialist unaware of the clinical presentation and mammographic result. Any focal uptake (or focal uptake within a breast with diffuse uptake) of 99mTc-MIBI in at least one planar image of the breast was the criterion for evaluating an image as suggestive of malignancy. Diffuse homogeneous or nonhomogeneous activity without focal accumulation was scored as equivocal (because it was impossible to state whether a small tumor could be present within the breast but was obscured by the physiologic uptake of 99mTc-MIBI). Homogeneous uptake of tracer in both breasts was classified as normal.
Confirmation of Pathology
All patients with suspicious breast lesions had core biopsy, fine-needle aspiration biopsy (FNAB), or definitive wide local excision to confirm the final diagnosis. Axillary node dissection was performed on 169 patients with confirmed malignancy of the breast. All histology and cytology slides were read by a specialist with an interest in breast cancer. If the results of biopsy indicated a benign lesion, follow-up physical examination and mammography were reviewed over the following year. The patient was classified as having no breast cancer only if the physical examination and mammography remained negative.
Data Analysis
Images were interpreted as true-positive when cancer was confirmed by the histologic examination. The scintimammography and mammography images were scored using five grades of certainty; these data were used to help construct the ROC curves. The images were scored as probably or definitely cancer (grade 4 or grade 5). A false-negative result occurred when cancer was present, but the images had been reported as definitely normal or benign, probably normal or benign, or equivocal (grades 1–3). The examination was interpreted as true-negative when cancer was excluded by histopathology and the images were scored as definitely or probably normal or benign (grades 1 and 2). A false-positive result was defined when the images were reported as probably or definitely cancer or equivocal (grades 3–5) but there was no malignant tumor. Results described as equivocal (grade 3) were always considered as incorrect because patients either did or did not have breast cancer on histologic examination. Combination imaging was defined as XMM followed by SMM; the combined result was determined by the highest score obtained with either modality in that patient (e.g., if XMM scored 2 [probably benign] and SMM scored 4 [probably malignant], the overall score was 4).
The ROC curves for XMM, SMM, and combined XMM and SMM imaging were composed using the same grading score for detection of cancer. Each point of the curve was evaluated to assess the false-positive and true-positive rates for grade 5, grades 5 + 4, and also grades 5 + 4 + 3. To compare the three techniques, we calculated the area under the ROC curve for each imaging technique and the results of combined imaging. Comparison was made with Wilcoxon statistics of the different areas with a signal-detection experiment (to differentiate true statistics from noise) using a method involving two-alternative forced choices (16–19).
RESULTS
The histologic samples obtained from mastectomy or excision biopsy led to a diagnosis of malignancy in 204 of 374 lesions (54.5%). Eight different histologic types of malignant tumors were identified; the different types identified and those with invasive ductal carcinoma were graded using the method of Bloom and Richardson (20) (Tables 1 and 2).
Results of Biopsy of Breast Lesions with Mean Age and Size of Tumor
Grades of 164 Invasive Ductal Carcinomas Studied Using Grading System of Bloom and Richardson by Age and Size of Tumor
99mTc-MIBI SMM diagnosed correctly 181 malignant lesions (Fig. 1). There were 23 breast cancers that were false-negative on SMM (including 3 of <10 mm). Of these breast cancers, 17 were reported as benign and 6 of them were evaluated as equivocal. False-positive uptake of 99mTc-MIBI was seen in 49 patients (35 reported as probably or definitely cancer and 14 reported as equivocal) with no cancer detectable on histologic examination or FNAB. Therefore, the sensitivity, specificity, PPV, and negative predictive value (NPV) of SMM were 89%, 71%, 79%, and 84% (Figs. 2 and 3, Table 3).
Overall Sensitivity, Specificity, PPV, and NPV and Area Under ROC Curve in XMM, SMM, and Combination

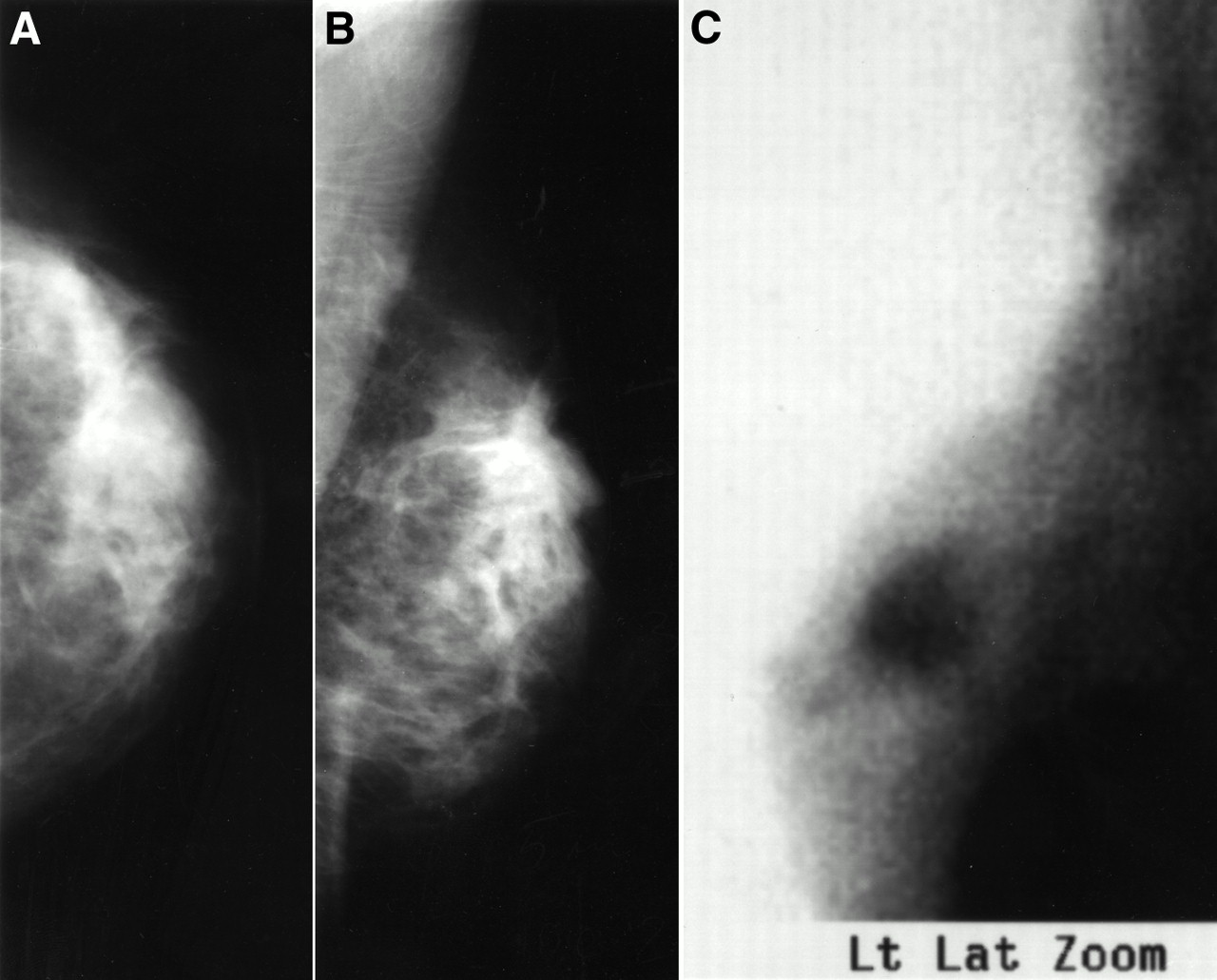
A 39-y-old patient with extensive palpable and dense left breast mass reported as equivocal on conventional two-view XMM (A and B) and reported as cancer on 99mTc-MIBI SMM (C). Invasive ductal carcinoma, Bloom–Richardson grade 2 (20), was confirmed on histologic examination.
A 30-y-old patient with palpable lesion reported as probably cancer (grade 4) on two-view XMM (A and B) but reported as normal on 99mTc-MIBI SMM (C). Histologic examination confirmed benign fibrocystic changes only.

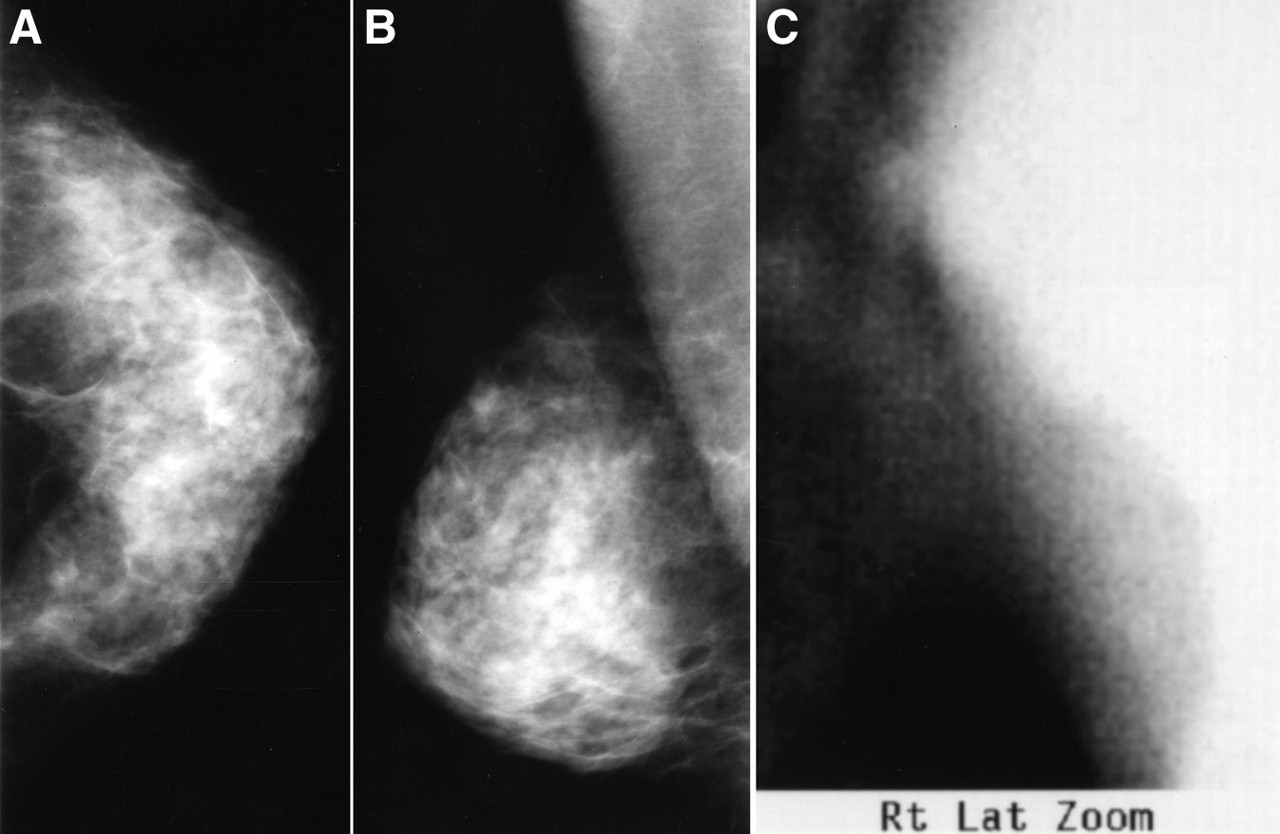
A 52-y-old patient with palpable lesion and right breast mass reported as normal (A and B); likewise, 99mTc-MIBI SMM (C) was reported as normal. Pathologic examination of excision biopsy specimen showed 20-mm grade 2 invasive ductal carcinoma.
XMM was able to identify 143 malignant breast cancers (70%); 61 cancers were reported as benign lesions (10 lesions) or equivocal (51 lesions). There were 117 true-negative studies. The sensitivity, specificity, PPV, and NPV of XMM for detection of breast carcinoma in this study were 70%, 69%, 73%, and 66%.
In subgroup analysis of 24 lesions evaluated histologically as ductal carcinoma in situ (DCIS), XMM was true-positive in 14 cancers (58%) and SMM detected 19 cancers (79%). The situation is not the same for lobular carcinoma in situ (LCIS), where there were nine lesions. SMM and XMM each detected seven sites of LCIS, but all nine lesions were seen by a combination of both modalities.
However, if combination of the two methods was used (XMM followed by SMM), sensitivity for identifying cancer was 93%, specificity was 72%, PPV was 80%, and NPV was 90% (Fig. 4). The ROC curves of the combined test show that the sensitivity was 80% and the specificity was 99% using the highest grade of certainty for cancer. If the upper three grades of certainty were used (grades 3–5), the sensitivity of the combined imaging was 93% with a specificity of 72%.
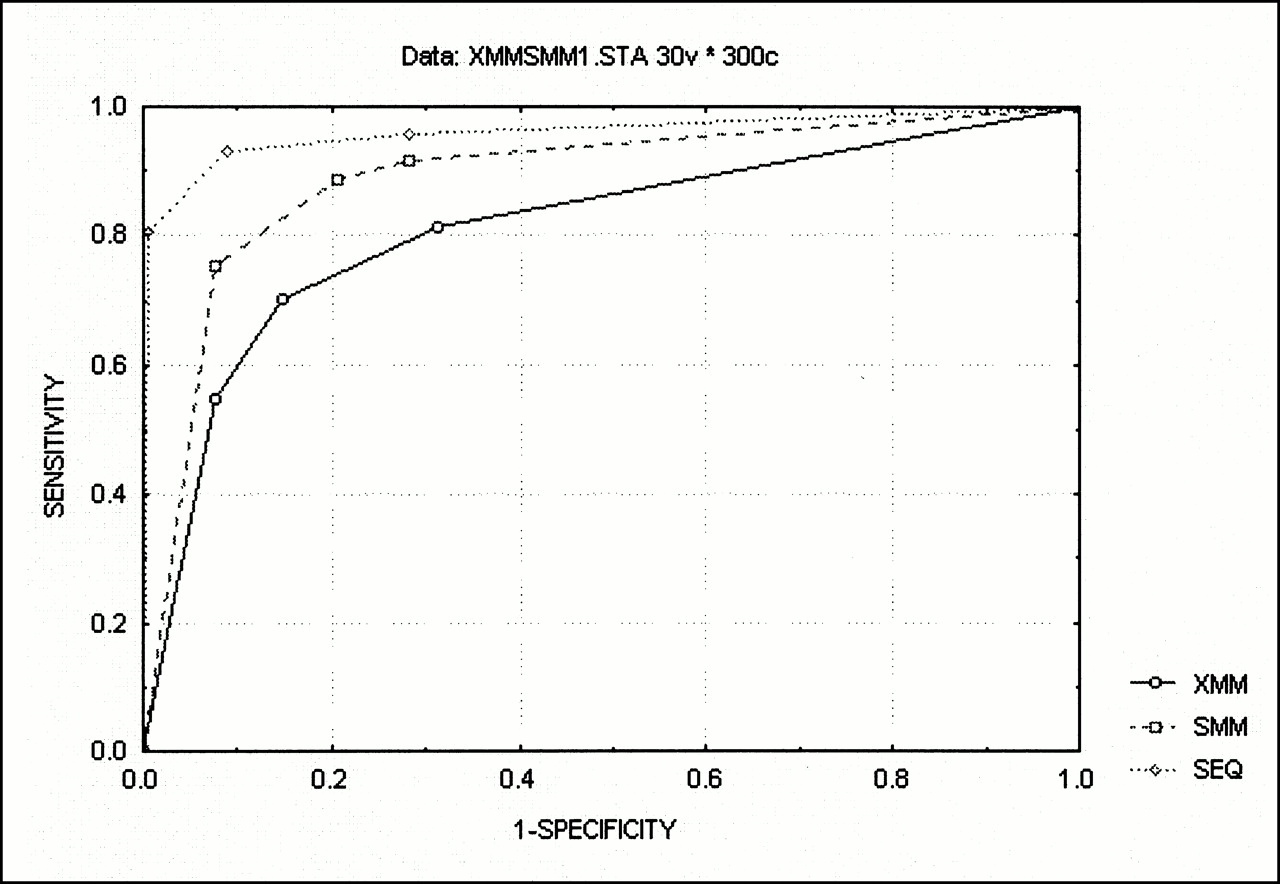
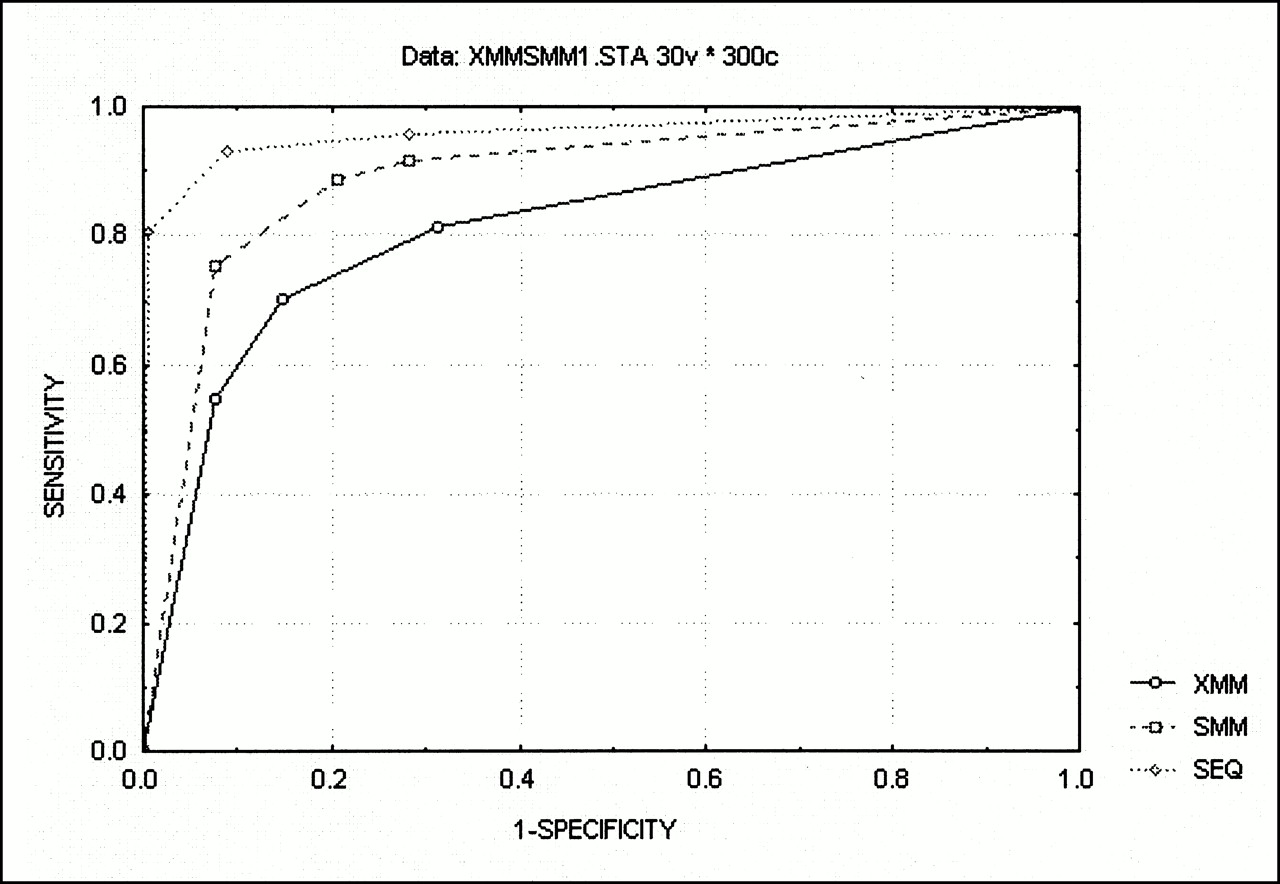
ROC curves for XMM, SMM, and combination of two techniques (SEQ).
Only nine cancers could not be seen with either modality. Six were invasive ductal carcinoma, two were DCIS (cribriform and solid), and one was a Paget’s cancer of the nipple.
The areas under the ROC curves for XMM, SMM, and combination imaging were XMM, 0.79; SMM, 0.85; and a combination of XMM and SMM, 0.93. Analysis of these areas under the ROC curves indicated no significant difference between SMM and XMM. Significant differences were found between SMM and sequence imaging and between XMM and sequence imaging (P < 0.05).
DISCUSSION
This study confirms the higher accuracy of SMM than XMM that has been reported in studies performed in many countries (5,9–14). One of the prime reasons may be the increased sensitivity of 99mTc-MIBI in most of these studies compared with that of XMM (10–14,21–25). However, specificity appears to be similar between the two techniques in most of these studies. This improvement of sensitivity is probably related to the qualitative nature of reporting XMM, in which the presence of malignancy is determined by the presence and the pattern of abnormalities in the breast (3,5). This appears to lead to a high number of equivocal reports, itself leading to uncertainty for the patient and the doctor. However, with SMM there are only two options: the presence or the absence of activity to give a positive or negative result. Therefore, the cancer can often be seen more clearly with SMM than with XMM. Single readers were used in this study because the primary aim was to test the accuracy of the two methods within a setting as close to clinical practice as possible. Comparing the ability of different readers to accurately read the XMM and SMM would be interesting but was outside the scope of this study. Also, at present, the criterion was that the positivity of 99mTc-MIBI SMM remains subjective. This will continue to be the case until a consensus can be formed regarding the best method for more objective reporting.
Although sonography is often thought to be the main second-line imaging test in breast cancer, it rarely provides information independent of the mammography because the sonography is directed by the mammography report. This makes an independent assessment of sonography versus XMM or SMM difficult. However, in our group it was often used to obtain tissue for cytologic or histologic assessment.
The uptake of any radiopharmaceutical into breast tissue depends initially on the vascularity of the tissue and then on a specific or nonspecific mechanism of uptake and retention of the radiopharmaceutical within the tumor (25–27). 99mTc-MIBI is retained within the mitochondria, and therefore the degree of uptake is related to the metabolic activity of the tumor (26). None of these factors is affected by factors such as breast density or scarring, which make reading mammography difficult. Therefore, the use of two complementary techniques imaging the breast from different aspects (anatomic and functional) provides the most accurate information.
Within certain subgroups, SMM seems to be at a particular advantage. For example, in DCIS the pickup from SMM was nearly twice that of XMM, possibly because not all sites of DCIS have sufficient calcification to be seen with ease. Lobular carcinoma and LCIS, unlike others types of cancers, often lack clinical and mammographic signs (1,3). In this group of lesions, which are particularly difficult to assess using standard XMM, we did not see any difference and good diagnostic accuracy was seen using either method.
It appears that the size of the lesion is less important than that reported in previous studies (9–12,21–24) because only three cancers of <10 mm were missed by SMM but the other cancers that were negative on SMM were much larger (10–30 mm). One clear difference is that in the group of patients studied in the United Kingdom (compared with most Northern European patients), women seem to present later in the course of their disease and the breast masses are larger at diagnosis (1,14). This will, therefore, improve the sensitivity of our data and, indeed, the figure of 89% in this study is in the upper range of that obtained in other studies. The reason for a negative SMM in the cancers of >10 mm was less clear and may be related to the differences in the biologic mechanism of uptake of 99mTc-MIBI into the cancer cells.
CONCLUSION
We have found that in the diagnosis of primary breast cancer, the addition of SMM to XMM gives a significant increase in the accuracy of breast imaging; this should provide an acceptable degree of certainty for diagnosis to allow SMM to be used as a routine second-line test in the investigation of breast cancer.
Acknowledgments
This work was supported by the Special Trustees of the Royal Free Hospital and grants from the International Atomic Energy Agency and the British Council. Part of this study was funded by the Research and Development fund of the National Health Service Executive. Dr. Buscombe has received research monies and honoraria from DuPont Pharma.
Footnotes
Received Mar. 15, 2000; revision accepted Jun. 20, 2000.
For correspondence or reprints contact: John R. Buscombe, MD, Department of Nuclear Medicine, Royal Free Hospital, London NW3 2QG, United Kingdom.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison between 99mTc-Sestamibi Scintimammography and X-ray Mammography in the Characterization of Clusters of Microcalcifications: A Prospective Long-term Study
- Integrin Receptor Imaging of Breast Cancer: A Proof-of-Concept Study to Evaluate 99mTc-NC100692
- Inconclusive Triple Diagnosis in Breast Cancer Imaging: Is There a Place for Scintimammography?
- New Technologies in Breast Imaging
- Diagnostic Value of 99mTc-Methylene Diphosphonate and 99mTc-Pentavalent DMSA Compared with 99mTc-Sestamibi for Palpable Breast Lesions
- Invited Commentary: One Step Forward
- Scintimammography