


Abstract
Esophagitis is a common complication of gastroesophageal reflux disease (GERD). Unfortunately, an accurate diagnosis of esophagitis usually requires invasive endoscopy. The purpose of our study was to evaluate the use of noninvasive 99mTc-methoxyisobutylisonitrile (MIBI) chest SPECT to detect esophagitis in GERD patients. Methods: Forty GERD patients who underwent endoscopy for diagnosis and grading of esophagitis according to the Savary–Miller grading system were included in this study. 99mTc-MIBI chest SPECT was performed on all patients to detect and grade esophagitis. Results: On the basis of the endoscopic findings, the sensitivity, specificity, and accuracy of 99mTc-MIBI chest SPECT to detect esophagitis were 100%, 77%, and 95%, respectively. The correlation between the Savary–Miller grading system and 99mTc-MIBI chest SPECT grading was found to be good. Conclusion: Noninvasive 99mTc-MIBI chest SPECT has excellent sensitivity and good accuracy as a screen for esophagitis.
Gastroesophageal reflux disease (GERD), defined as symptoms or as tissue damage resulting from the reflux of gastric contents into the esophagus, is a common medical problem (1). Esophagitis is the most prevalent complication of GERD, affecting >40% of GERD patients, and has therapeutic implications (2). The clinical usefulness of a reliable, noninvasive technique such as barium radiography for diagnosing esophagitis is obvious, but it is relatively insensitive. Invasive endoscopy is still the gold standard for diagnosing esophagitis and is the routine practice. The use of radiopharmaceuticals has been investigated as a noninvasive means of detecting esophageal pathology. 67Ga imaging has been used to detect candidal esophagitis (3). 99mTc-pertechnetate has been used to identify Barrett's esophagus (4). However, the poor sensitivity and negative predictive value limit its use as a screening test (5). A review of the literature indicated that 201T1 SPECT had a high sensitivity to detect esophagitis compared with the endoscopic findings (6). However, poor emission characteristics for SPECT imaging and availability problems related to cyclotron production are significant disadvantages of 201T1. Thus, there has been a continuous effort to find an imaging agent that can be labeled with 99mTc that is readily available and has the attractive nuclear properties of 99mTc that would be suitable for SPECT imaging.
Recently, noncardiac applications of 99mTc-methoxyisobutylisonitrile (MIBI) chest SPECT showed it could be helpful to detect lung and esophageal cancers (7,8). Furthermore, using 99mTc-MIBI chest SPECT to detect coronary artery disease, the authors noted increased uptake in the esophagus of one patient with esophagitis (9). On the basis of this observation, the purpose of our study was to evaluate 99mTc-MIBI SPECT as a potential noninvasive method to detect esophagitis in GERD patients.
MATERIALS AND METHODS
Participants
A total of 40 patients (16 women, 24 men; age range, 30–65 y; mean age, 47.0 ± 10.7 y) with suspected GERD were enrolled in our study. Each patient was interviewed by a qualified gastroenterologist and was asked to complete a questionnaire regarding symptoms suggestive of GERD, including heartburn, chest pain, dysphagia, odynophagia, nausea, vomiting, and acid regurgitation (10,11), for at least 3 mo before the study. We also evaluated a group of 30 healthy volunteers (control subjects) (12 women, 18 men; age range, 28–68 y; mean age, 48.2 ± 11.5 y) without suspected GERD and with negative endoscopic findings. All participants with a history of smoking, previous upper gastrointestinal surgery, or cardiopulmonary, immunorheumatic, endocrine, hepatobililary, urinary, and other systemic diseases were excluded. All participants were asked to refrain from drugs, including alcohol, coffee, and tea, for at least 1 wk. The esophagus was then carefully evaluated, and the extent of mucosal injury was determined on the basis of endoscopic findings. Negative findings were defined as grade 0, and positive findings were defined according to the Savary–Miller grading system (12): grade 1, linear, nonconfluent erosions; grade 2, longitudinal, confluent, noncircumferential erosions; grade 3, longitudinal, confluent, circumferential erosions that bleed easily; and grade 4, esophageal ulceration or stricture. In this study, the patients and control subjects were from our health centers; endoscopy and 99mTc-MIBI SPECT were suggested and performed with permission from the patients and control subjects.
99mTc-MIBI Chest SPECT
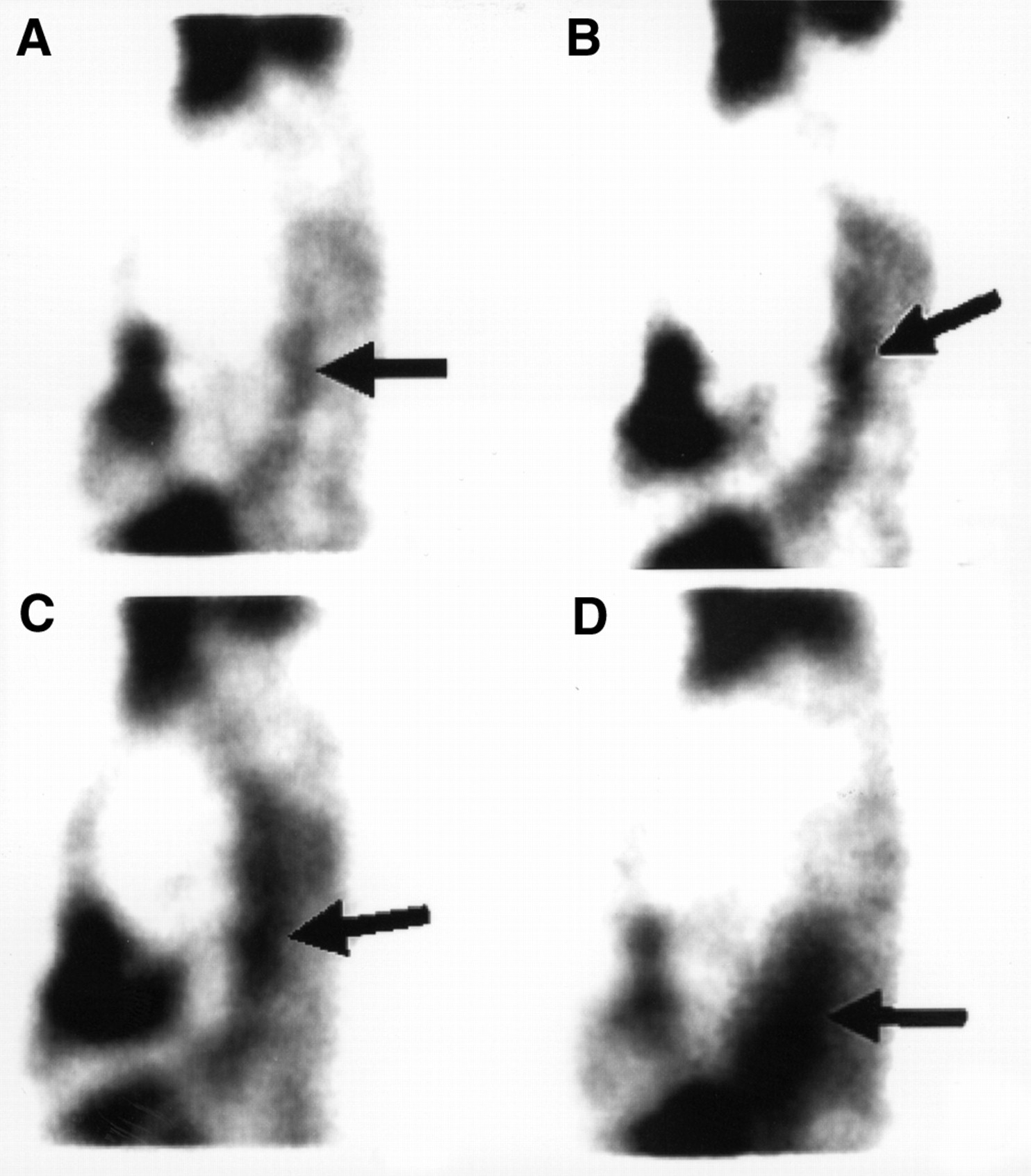
On the morning after endoscopy, patients were scheduled for 99mTc-MIBI chest SPECT after an overnight fast of >8 h and a waiting period of 30 min after oral intake of 500 mg perchlorate to prevent abnormal uptake of free 99mTc-pertechnetate. Cardiolite, a commercial MIBI preparation (maximum, 5.56 GBq [150 mCi] in ∼1–3 mL) was obtained from Dupont Pharmaceuticals (Billerica, MA). The labeling and quality control procedures were performed according to the manufacturer's instructions. Labeling efficiency was always >90%. Chest SPECT was performed 10 min after an intravenous injection of 740 MBq (20 mCi) 99mTc-MIBI. The patient was positioned supine on the imaging table with the chest strapped to prevent motion. The equipment consisted of a rotating, large field-of-view gamma camera (Apex 609R; Elscint Ltd., Haifa, Israel) fitted with a low-energy, high-resolution collimator. Sixty images were acquired for 10 s each during a 360° camera rotation. Each image was stored in a 64 × 64 pixel matrix. Reconstruction of the image was performed with attenuation correction, using Hann filters (cutoff frequency, 1.0) to produce SPECT images. All projections for each chest SPECT examination were reviewed and interpreted by 2 or more nuclear medicine physicians who were unaware of the endoscopic findings. The slices of SPECT were interpreted as negative (grade 0, no uptake in the esophagus) or positive (grade 1, slight esophageal uptake and significantly less than that of the heart; grade 2, mildly esophageal uptake and not significantly less than that of the heart; grade 3, moderate esophageal uptake and equal to that of the heart; and grade 4, substantial esophageal uptake and greater than that of the heart) (Fig. 1).
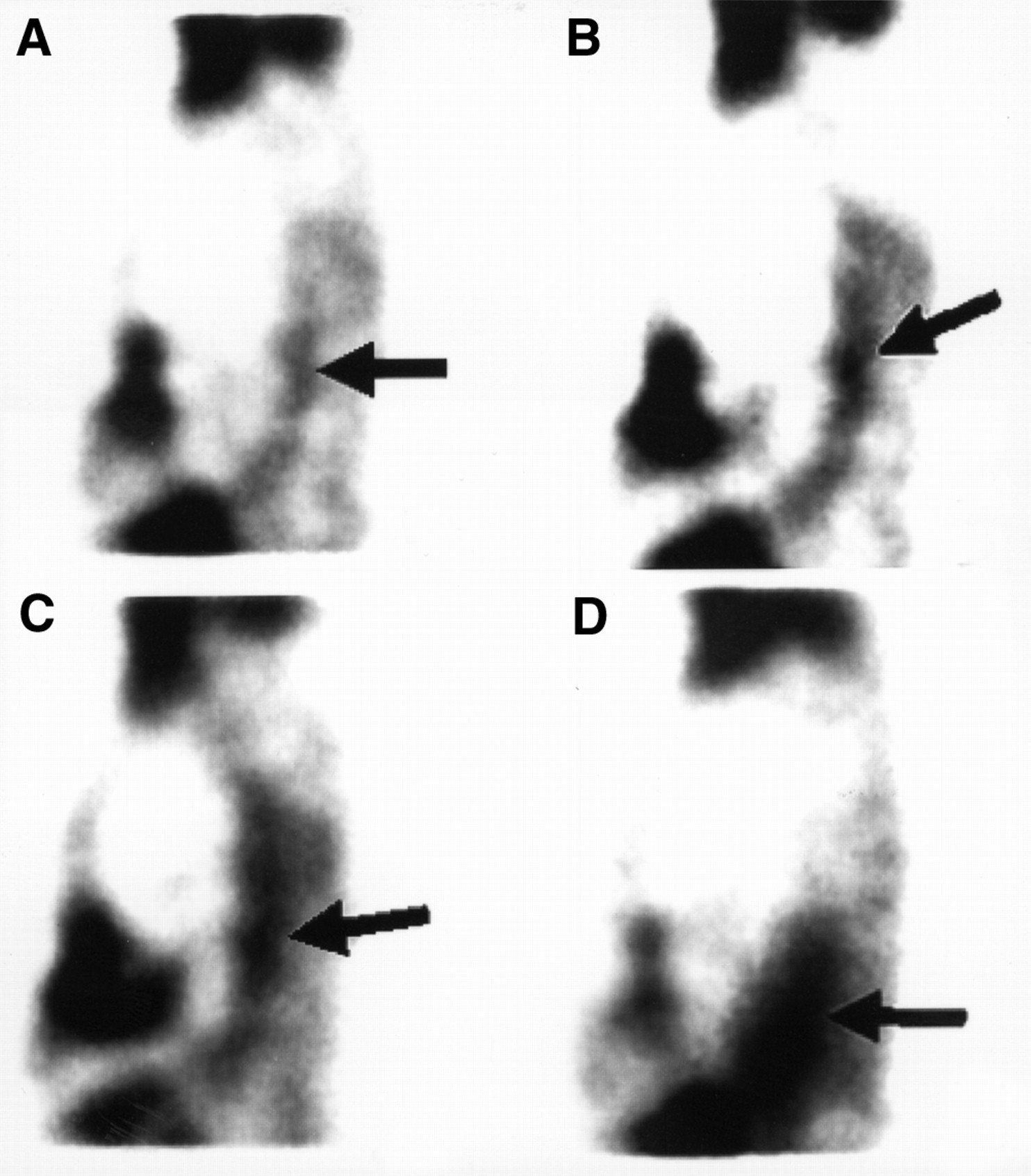
Sagittal slices of SPECT were interpreted as positive: grade 1 (A), grade 2 (B), grade 3 (C), and grade 4 (D). Arrows indicate location of esophagitis.
Statistical Analysis
In accordance with the endoscopic findings, the sensitivity, specificity, and accuracy of 99mTc-MIBI chest SPECT to detect esophagitis were determined. The agreement between the Savary–Miller grading system based on endoscopic findings and grading from 99mTc-MIBI chest SPECT was evaluated on 5 × 5 contingency tables using Spearman rank order correlation (TSTATISTICA for Windows; StatSoft, Inc., Tulsa, OK). Two-tailed P values < 0.05 were considered to be statistically significant.
RESULTS
Detailed patient data including endoscopic findings versus 99mTc-MIBI chest SPECT findings are listed in Table 1 and Figure 2. All 30 healthy controls had negative 99mTc-MIBI chest SPECT findings. The sensitivity, specificity, and accuracy of 99mTc-MIBI chest SPECT for detection of esophagitis were 100% (95% confidence interval [CI], 0.89–1.00), 77% (CI, 0.40–0.97), and 95% (CI, 0.83–0.99), respectively. The 5 × 5 contingency table used to evaluate the agreement between the Savary–Miller grading system and 99mTc-MIBI chest SPECT grading is presented as Table 2. The correlation was good (r = 0.919, P < 0.001).
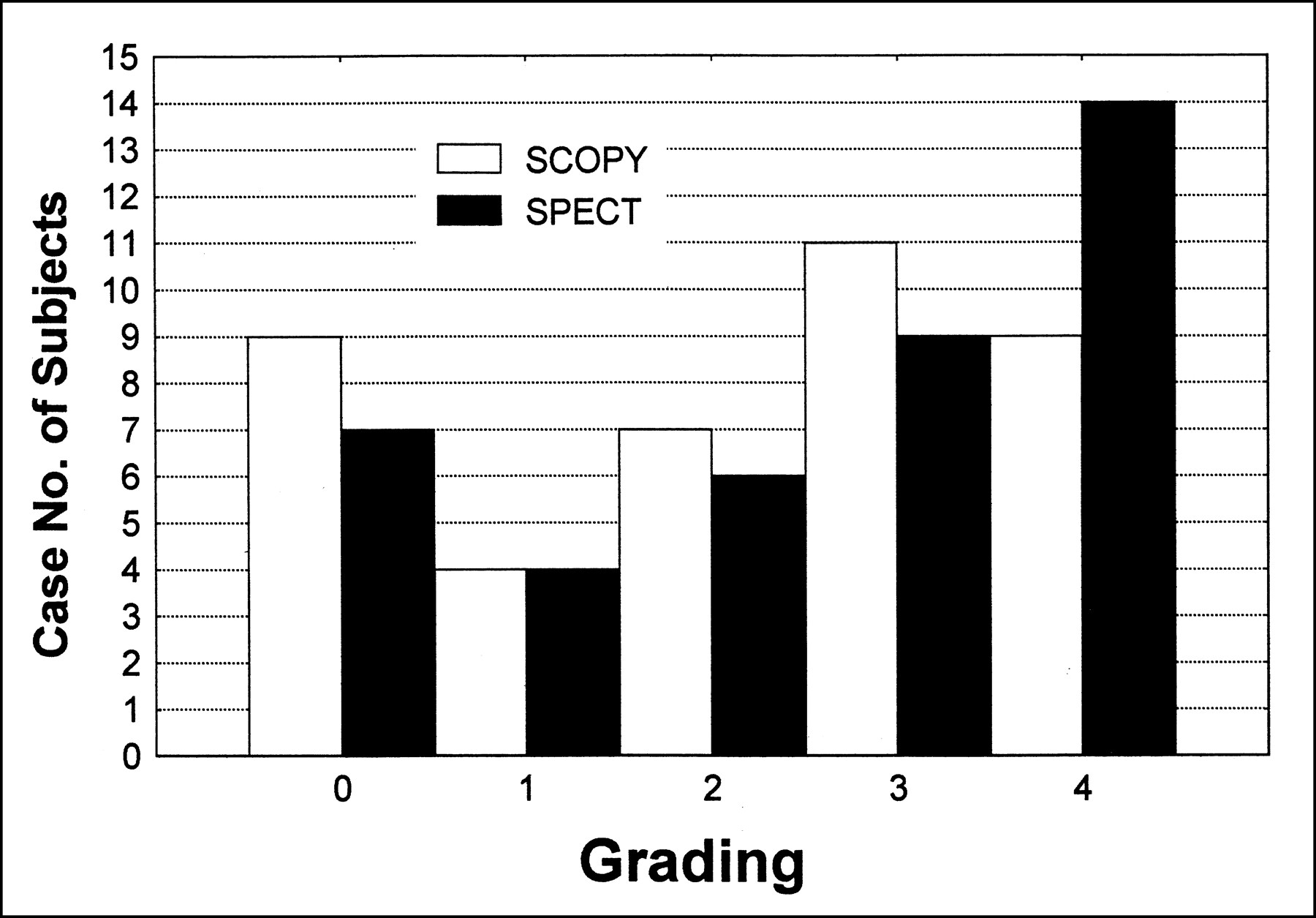
Histogram of endoscopic grading versus 99mTc-MIBI chest SPECT grading. SCOPY = endoscopy.
Patient Data with Endoscopic Findings and 99mTc-MIBI Chest SPECT Findings
Relationship Between Savary–Miller Grade and 99mTc-MIBI Chest SPECT Grade
DISCUSSION
Esophagitis associated with GERD has been commonly reported in the highly developed countries, such as Switzerland (11.7%), the United States (15.7%), and the United Kingdom (22.8%) (13). Heartburn and acid regurgitation are specific for GERD when they are the predominant symptoms. However, invasive endoscopy is still the gold standard that is useful for evaluating the severity of esophagitis (14).
Tc-MIBI is available in kit form, ready to be labeled with 99mTc. It has the distinct advantage that patients can be imaged as early as 10 min after injection. It is ideally suitable for SPECT imaging. 99mTc-MIBI, a member of the isonitrile class of coordination compounds, is a lipophilic cation used for myocardial perfusion imaging. The mechanism of 99mTc-MIBI uptake in esophagitis is not yet clearly understood. Mitochondrial or plasma membrane potentials and cellular mitochondrial content of esophageal mucosa and inflammatory cells could all play a significant role in uptake of 99mTc-MIBI (15,16) in esophagitis, or the uptake may be caused by indirect phenomena such as locally increased blood flow and capillary permeability from inflammation. Therefore, the hypothesis underlying this study was that increased blood flow and capillary permeability associated with esophageal erosions or inflammation could be detected by 99mTc-MIBI chest SPECT imaging.
The biodistribution of 99mTc-MIBI is characterized by rapid blood clearance and, consequently, an early uptake by target organs (17). The early imaging time of esophageal lesions (8) at 10 min after intravenous injection of 99mTc-MIBI was adequate in our study. Therefore, we did not obtain 1- or 2-h images in our clinical practice. Because all projections for each chest SPECT examination were reviewed by at least 2 nuclear medicine physicians, the possibility of false-positively detecting esophagitis associated with the inference of myocardial radioactivity scarring from predominant cardiac uptake of 99mTc-MIBI (18) was avoided. In addition, to decrease false-positive findings from swallowed saliva containing free 99mTc-pertechnetate or abnormal esophageal mucosa uptake of free 99mTc-pertechnetate, the pretreatment of patients with sodium or potassium perchlorate was necessary in this study. Perchlorate is a monovalent negative ion of approximately the same ionic size as 99mTc-pertechnetate. It blocks abnormal uptake of free pertechnetate in salivary glands and esophageal mucosa by competitive inhibition (19). No cases of false-negative SPECT findings but two cases of false-positive SPECT findings were found in our study. Although enterogastric bile reflux during 99mTc-MIBI imaging (20,21) might have induced false-positive findings in our study, the endoscopic examinations of our patients revealed no definite bile reflux into the stomach or esophagus. After reviewing the endoscopic findings of the two false-positive cases, mild esophageal varices were considered to be the possible cause of false-positive SPECT findings because of blood pooling in the engorged vessels.
Although this pilot study population is small, 99mTc-MIBI chest SPECT appears to have high sensitivity and accuracy to detect esophagitis in GERD patients. We did not perform the correction of esophagitis sizes between endoscopic and SPECT findings because we used the Savary–Miller grading system (12) to grade esophagitis in this study.
CONCLUSION
99mTc-MIBI SPECT for exclusion of coronary artery disease is excellent when chest pain is encountered. If uptake in the esophagus can be seen in early postexercise or rest studies, the next examination should be endoscopy. This method can be used as a follow-up and control after an esophageal carcinoma has been ruled out.
Footnotes
Received Dec. 28, 1999; revision accepted May 16, 2000.
For correspondence or reprints contact: Chia-Hung Kao, MD, Department of Nuclear Medicine, Taichung Veterans General Hospital, 160 Taichung Harbor Rd., Section 3, Taichung 407, Taiwan.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.