


Abstract
Carcinoid tumors can produce serotonin (5-hydroxytryptamine) and catecholamines from the precursors tryptophan and tyrosine. Our aim was to evaluate the tyrosine analog l-3-[123I]iodo-α-methyltyrosine (IMT) in the detection and the determination of biochemical activity of these tumors in comparison with 111In-labeled [diethylenetriaminepentaacetic acid (DTPA)-d-Phe1]-octreotide (111In-octreotide) scintigraphy. Methods: SPECT and planar whole-body imaging were performed 15 min after administration of 300 MBq IMT in 22 patients with metastatic carcinoid tumors. The number of lesions detected was compared with the number detected by 111In-octreotide scintigraphy. The size and intensity of uptake of all lesions were graded using a simple scoring system, yielding a total body uptake score for both tracers. These scores were compared (nonparametric correlation) with biochemical markers of serotonin and catecholamine metabolism. Results: IMT SPECT detected only 63 of 145 lesions detected by 111In-octreotide imaging (43%). IMT SPECT performance was best in the liver (60% detection rate). Both IMT uptake and 111In-octreotide uptake scores correlated with markers of serotonin metabolism (respective values for urinary 5-hydroxyindoleacetic acid: r = 0.67 and 0.48, P < 0.001 and 0.05; for urinary serotonin: r = 0.56 and 0.40, P = 0.002 and 0.05; and for platelet serotonin: r = 0.57 and 0.45, P < 0.01 and 0.05). No correlation with adrenaline or noradrenaline metabolites was found. However, IMT uptake, but not 111In-octreotide uptake, correlated with dopamine metabolite excretion (homovanillic acid: r = 0.60, P < 0.05; and dopamine relative sum: r = 0.61, P < 0.05). IMT uptake was higher in patients with increased dopamine metabolite excretion (P = 0.05). Conclusion: IMT uptake can be demonstrated in carcinoid lesions, but the method detected only 43% of carcinoid lesions that were positive on 111In-octreotide scintigraphy. Uptake of both tracers is related to the serotonin secretory activity. However, IMT uptake, but not 111In-octreotide uptake, was related to tumor dopamine metabolism. These findings may be of interest in the metabolic targeting of carcinoids.
Carcinoid tumors are neuroendocrine tumors that can occur anywhere in the human body and are traditionally described as originating from the foregut, midgut, or hindgut (1). These tumors are thought to be derived predominantly from enterochromaffin cells. These cells possess the specific property to take up and decarboxylate amine precursors and usually produce a variety of peptides and biogenic amines, of which serotonin (5-hydroxytryptamine) is the most prominent (2). When these generally slowly growing tumors have metastasized, secretory products are no longer subject to primary metabolization in the liver, enter the systemic circulation, and can cause the carcinoid syndrome (3). This syndrome is characterized by flushing, diarrhea, and, less commonly, wheezing, right heart-valve fibrosis, or pellagra (4,5). These symptoms are often the first clinical manifestation of the tumor, although in some cases the primary tumor in the abdomen may cause early mechanical symptoms (4). When the disease has metastasized, partial liver resection or transplantation may be curative in selected patients, but, in general, curative treatment (surgery) is no longer possible (6). Treatment is then aimed at tumor load reduction, inhibition of secretion, and symptom management (7).
Biochemical measurement of secretory products and imaging studies are important investigations in diagnosing and staging carcinoid tumors. Biochemical measurements include analysis of metabolites from the serotonin and catecholamine metabolic pathways and measurement of various gut hormones. Quite specific for the often dominating serotonin secretion is measurement of urinary 5-hydroxyindoleacetic acid (5-HIAA), the main serotonin metabolite (Fig. 1). Imaging of carcinoids has greatly improved since the introduction of somatostatin receptor scintigraphy with 111In-labeled [diethylenetriaminepentaacetic acid (DTPA)-d-Phe1]-octreotide (111In-octreotide). Together with various radiologic methods (CT, sonography), 111In-octreotide scintigraphy is a reliable and effective method to visualize carcinoid tumor locations throughout the body (8–10).
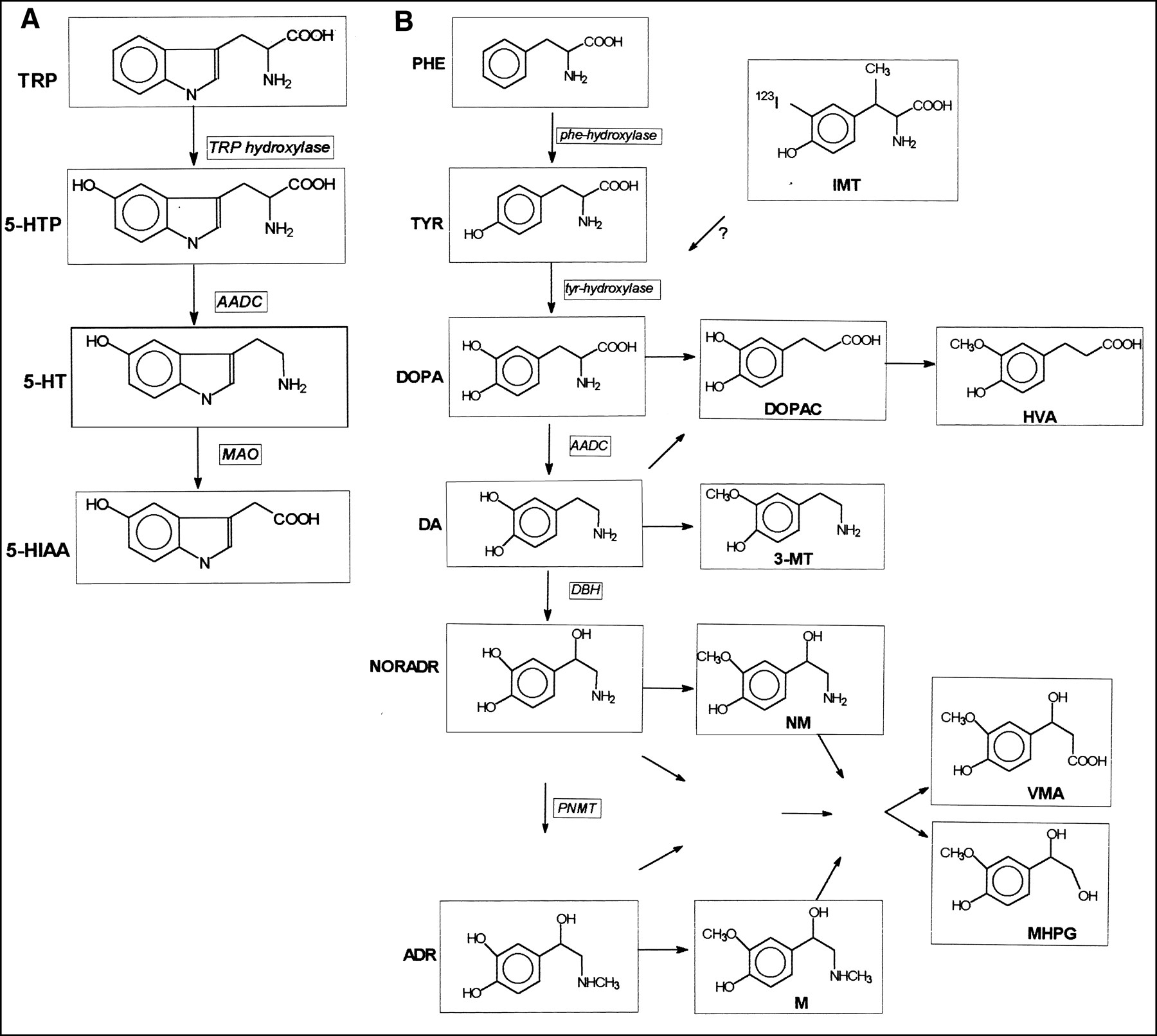
Major steps in serotonin metabolism (A) and simplified overview of catecholamine metabolism (B) show only most important enzymes and metabolites. TRP = tryptophan; 5-HIAA = 5-hydroxyindolacetic acid; AADC = aromatic l-amino acid decarboxylase; MAO = monoamine oxidase; PHE = phenylalanine; TYR = tyrosine; DOPA = 3,4-dihydroxyphenylalanine; DA = dopamine; NORADR = noradrenaline; ADR = adrenaline; DOPAC = 3,4-dihydroxyphenylacetic acid; 3-MT = 3-methoxytyramine; HVA = homovanillic acid; NM = normetanephrine; M = metanephrine; VMA = vanillylmandelic acid; MHPG = 3-methoxy-4-hydroxyphenylethylene glycol; DBH = dopamine-β-hydroxylase; PNMT = phenylethanolamine-N-methyltransferase.
Despite improved imaging, the effects of treatment are difficult to monitor. Although 111In-octreotide scintigraphy is effective in staging, conflicting data exist regarding the relation between somatostatin receptor expression and secretory activity: Although secretory activity clearly decreases under nonradioactive octreotide therapy, the uptake of 111In-octreotide is unaffected or may even increase (11,12). Radiologic techniques are also less reliable for monitoring treatment effects because the size of carcinoid lesions often does not change despite metabolically effective therapy (13). Therefore, the search continues for better methods to detect and evaluate treatment effects on these tumors. Methods using radiolabeled metabolic precursors are potentially suitable for this purpose.
Radionuclide imaging using l-3-[123I]iodo-α-methyltyrosine (IMT), a modified amino acid that is avidly taken up in many malignant tumors, could therefore be of interest (14,15). The uptake of this agent is mediated through amino acid transport systems (16,17). Transmembrane transport of amino acids has to be greatly increased in actively secreting carcinoid tumors. Usually the amino acids tryptophan (precursor for serotonin synthesis) (Fig. 1A) and tyrosine (precursor for catecholamine synthesis) (Fig. 1B) share the same membrane transporter (18). Because IMT also enters cells through this transporter as an analog of tyrosine (16,17), the artificial amino acid IMT might be taken up in carcinoid tissue, especially when catecholamines are produced.
Therefore, we performed a study in patients with metastasized carcinoid tumors to assess whether IMT is taken up in these lesions and, if so, whether uptake is related to serotonin and catecholamine secretory activity. 111In-octreotide scintigraphy was used as the reference method for lesion detection. Secretory activity was assessed by biochemical analyses of blood and urine for serotonin, catecholamines, and their metabolites.
MATERIALS AND METHODS
Patients
Twenty-two patients (10 men, 12 women; mean age, 63 y; age range, 43–76 y) with a metastasized carcinoid tumor of midgut (n = 20) or hindgut (n = 2) origin were included in the study. The primary carcinoid tumor had been removed in all patients. All patients had a histologically proven carcinoid tumor in at least 1 location. Patients were recruited between August 1997 and February 1999 at the outpatient clinic of the Groningen University Hospital with a referral function in diagnosis and treatment of carcinoid tumor patients. Symptoms and use of medications were noted at inclusion. All medications were continued during the period of the IMT and 111In-octreotide study and during biochemical measurements. Written informed consent was obtained from all patients. The study was approved by the medical ethics committee of the Groningen University Hospital.
IMT Synthesis
Synthesis of IMT was performed as described by Krummeich et al. (19) with minor modifications. Briefly, IODO-GEN (Pierce, Rockford, IL) iodination with Na123I (t1/2 = 13.2 h; Amersham Cygne, Eindhoven, The Netherlands) of the precursor l-α-methyltyrosine was performed in a borate buffer. IMT was purified by elution with saline containing 5% ethanol over a C18 SepPak cartridge (Waters, Milford, MA) preconditioned with 100% ethanol followed by saline containing 5% ethanol. After filtration through a sterile 0.22-μm Millex GV filter (Millipore, SA, Molsheim, France), a colorless, ready-to-inject solution was obtained. Samples were shown to be sterile and pyrogen free. Quality control was performed by high-performance liquid chromatography on an RP-18 Multisorb 100 × 4.6 mm column (Pharmacia, Woerden, The Netherlands) using a mixture of H2O, ethanol, and acetic acid (87.5:10:2.5 [volume/volume/volume%]) as eluent. Radiochemical purity was >99% in all cases; specific activity was ∼11.1 TBq/mmol. The overall synthesis time, including purification and quality control, was <1 h. The radiochemical yield was 50%–65%. The reported effective dose equivalent is 2 mSv (20).
IMT Imaging
After at least a 5-h fast, SPECT imaging of the abdomen was performed 15 min after the intravenous injection of 250–300 MBq IMT. Fifteen minutes before tracer injection, 10 drops of Lugol's solution were given orally to prevent thyroid uptake of possibly formed free 123I. After SPECT, a whole-body scan was acquired using 3 adjacent spot views. A large field-of-view, double-head gamma camera (MULTISPECT 2; Siemens Inc., Hoffman Estates, IL) was used with a medium-energy, all-purpose collimator and a 15% window centered on the 159-keV photopeak of 123I. System resolution was 12-mm full width at half maximum at a 10-cm distance.
IMT SPECT included 64 projections (2 × 32; 5.6°/step) of 30-s duration each in a 128 × 128 matrix format. Spot views lasted 10 min and were recorded in a 128 matrix. The total scan procedure took ∼60 min. Transaxial tomograms were reconstructed without prefiltering using filtered backprojection with a Butterworth filter of sixth order and a cutoff frequency of 0.275 Nyquist. Attenuation correction was performed for abdominal SPECT studies using Chang's method with an attenuation coefficient of 0.11/cm.
111In-Octreotide Imaging
Twenty-four hours after administration of 200 MBq 111In-octreotide (Octreoscan; Mallinckrodt, Petten, The Netherlands), planar total-body scans (3 spot views of 10 min in a 128 matrix) were obtained using the same camera/collimator system as that used for the IMT studies. Both 173- and 247-keV photopeaks of 111In were used (15% windows for each). In addition, SPECT acquisition and processing were performed using the same specifications as those for IMT with the exception of a Butterworth cutoff filter frequency of 0.35. Additional 48-h images were recorded, when necessary, because of interfering bowel activity
111In-octreotide imaging was performed within 14 d of the IMT scanning in 17 patients. In 12 of these patients, 111In-octreotide was administered immediately after the end of the IMT procedure with imaging on the next day. The preceding IMT scanning did not alter 111In-octreotide images because of the rapid excretion of IMT and the lack of significant overlap between the 123I and the 111In windows. In the 5 patients with longer intervals (14, 26, 52, 85, and 120 d), we verified that no change in medical treatment had been introduced, no operations had been performed, the entire disease progression was slow in comparison with the interval, and biochemical secretory activity had not changed.
Image Interpretation
All IMT and 111In-octreotide images were read without knowledge of other imaging and biochemical information. For both tracers, the number of lesions was scored for 3 region categories: liver, abdominal, and extra-abdominal. An uptake score was established for each lesion, with uptake intensity and lesion size graded as follows: 1 point, small lesion (<2 cm) with low uptake (slightly more than normal liver uptake); 2 points, either small lesion with intense uptake (clearly more than normal liver uptake) or large lesion (2–5 cm) with low uptake; and 3 points, large lesion with intense uptake. Size estimations were based on CT or sonographic data. When lesions appeared to be >5 cm or confluent, they were considered to be made up of 5-cm-unit lesions, and >1 lesion could be scored. In this way, a simple semiquantative uptake score was established by grading the amount of whole-body tumor uptake for both tracers. 111In-octreotide imaging was considered as a gold standard for the presence of lesions.
Biochemical Measurements
As biochemical parameters for serotonin metabolism, urinary 5-HIAA, serotonin in a 24-h urine collection, and serotonin levels in platelets were measured (Fig. 1A). Measurement of serotonin in platelets is less influenced by dietary serotonin and is more sensitive for the detection of serotonin overproduction than is 5-HIAA up to intermediate 5-HIAA levels (21–23). Catecholamines are dopamine, adrenaline, and noradrenaline. Catecholamine metabolites were analyzed in 2 groups: the first group includes metabolites from dopamine, and the second group includes metabolites from adrenaline and noradrenaline (Fig. 1B). Parameters for dopamine metabolism were urinary levels of 3,4-dihydroxyphenylacetic acid (DOPAC), dopamine, homovanillic acid (HVA), and 3-methoxytyramine (3-MT) (24). In addition, a dopamine relative sum was defined as the sum of DOPAC, HVA, and 3-MT levels, each divided by their upper normal values. It should be noted that the urinary dopamine concentration itself is influenced by renal dopamine production from other catecholamine metabolites. Parameters for adrenaline and noradrenaline metabolism were urinary levels of adrenaline, noradrenaline, metanephrines and normetanephrine, vanillylmandelic acid (VMA), and 3-methoxy-4-hydroxyphenylethylene glycol (MHPG). Measurements were performed as described (25,26). Catecholamine metabolites were determined in hydrolyzed urine samples and thus represent free and conjugated fractions. Catecholamines were determined as free fraction. Upper reference limits were as follows: 5-HIAA, 3.8 mmol/mol creatinine; serotonin in platelets, 5.4 nmol/109 platelets; urinary serotonin, 66 μmol/mol creatinine; 3-methoxytyramine, 170 μmol/mol creatinine; noradrenaline, 30 μmol/mol creatinine; adrenaline, 10 μmol/mol creatinine; dopamine, 300 μmol/mol creatinine; metanephrines, 70 μmol/mol creatinine; normetanephrines, 260 μmol/mol creatinine; HVA, 5.5 mmol/mol creatinine; DOPAC, 2.0 mmol/mol creatinine; VMA, 2.5 mmol/mol creatinine; and MHPG, 1.5 mmol/mol creatinine.
Biochemical analysis was performed within 1 mo of the 111In-octreotide and IMT scintigraphy. All 3 markers of serotonin metabolism were available for all patients. One or more valid markers of catecholamine metabolism were available in 19 of 22 patients. Valid dopamine markers were available in 13 patients. Missing values were caused by logistic problems regarding reliable urine sampling or intervals between measurement and scans in which the secretory pattern was not in steady state.
Statistics
The number of lesions in each patient and the uptake scores using both tracers were compared nonparametrically with parameters of serotonin, catecholamine, and dopaminergic metabolite levels using the Spearman correlation coefficient. Subgroups (catecholamine-secreting carcinoid patients, patients on medication) were compared using the Mann-Whitney U test. The significance level was P ≤ 0.05.
RESULTS
Table 1 summarizes patient characteristics. In all 22 patients, 1 or more lesions were found on 111In-octreotide imaging. In 18 of these patients, IMT SPECT detected abnormalities (patient-based sensitivity, 82%). In total, 145 lesions were detected by 111In-octreotide imaging, of which 63 were found to be positive on IMT imaging (overall lesion-based sensitivity, 43%). On average, 6.6 lesions were found in each patient using 111In-octreotide, and 2.9 lesions were found using IMT. The detection rate of IMT SPECT was best in the liver (42/70 lesions; sensitivity, 60%). In the extrahepatic abdomen, only 9 of 44 (21%) lesions were scored positive on IMT imaging; in the extra-abdominal area, 12 of 32 (38%) lesions were scored positive. In all patients, 111In-octreotide images were of better quality because of higher contrast between lesion and background. Carcinoid lesions that were negative on IMT imaging but positive on 111In-octreotide imaging were both small and large. Examples are shown in Figures 2 and 3. No lesions with evident IMT uptake were negative on 111In-octreotide imaging.

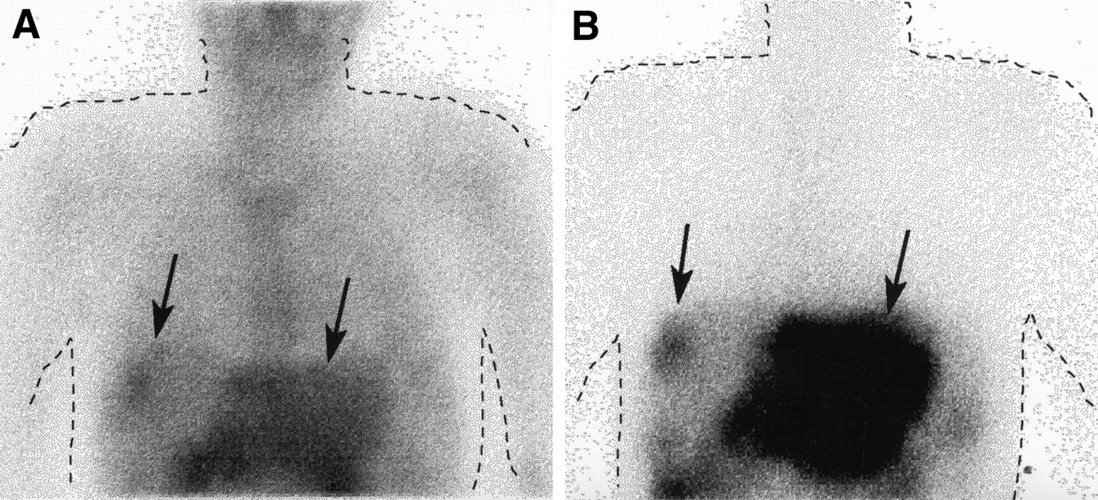
Planar images of liver and chest in patient with small lesions of midgut carcinoid (arrows) in right liver lobe and large lesion including entire left lobe. IMT image (A) and 111In-octreotide image (B) show same uptake pattern but higher contrast for 111In-octreotide.

Planar images of abdomen in patient with metastases from midgut carcinoid tumor in mediastinum, para-aortic region, and mesentery. (A) IMT image shows no uptake. (B) 111In-octreotide image reveals intense lesion uptake (arrows).
Patient Characteristics, Biochemical Markers, and Tracer Uptake Scores
On IMT images, the 8 patients using secretion-inhibiting medication (unlabeled octreotide or interferon-α) tended to have more lesions (4.0 ± 3.3 versus 1.8 ± 2.0; not significant) and higher uptake scores (5.8 ± 3.8 versus 4.1 ± 3.7; not significant) compared with patients without this medication. However, the difference was not significant. On 111In-octreotide images, these medication users had significantly more lesions (10.1 ± 3.5 versus 4.6 ± 3.2; P < 0.01) and higher uptake scores (17.6 ± 8.4 versus 7.7 ± 6.0; P < 0.01).
Twenty patients had biochemical evidence of increased serotonin secretory activity (Table 1). Eleven of these also had increased levels of catecholamine metabolites. In 8 of these 11 catecholamine-producing carcinoids (especially dopamine metabolites), excretion was increased (Fig. 1). All 16 patients who were troubled by symptoms of the carcinoid syndrome had hypersecretion of serotonin. Three patients had abdominal pains. Three patients were completely asymptomatic: 1 had no hypersecretion, 1 had serotonin hypersecretion but used medication, and 1 had evident hypersecretion but no carcinoid syndrome.
Despite the low detection rate of IMT for carcinoid lesions, significant correlations were found between tumor IMT uptake and all 3 biochemical parameters of serotonin secretory activity (Table 2, Fig. 4). Significant, but lower, correlations with serotonin metabolism were present for the 111In-octreotide uptake score. No correlations were found with catecholamine metabolites from adrenaline and noradrenaline. However, IMT uptake, but not 111In-octreotide uptake, correlated with excretion of dopamine metabolites (Table 2). Furthermore, IMT uptake scores were higher in the dopamine-secreting subgroup than in those patients without elevated dopamine metabolites (6.0 ± 4.5 versus 2.4 ± 3.0; P = 0.05).

Scatter plot shows relation between IMT uptake and urinary 5-HIAA excretion (A), serotonin platelet level (B), urinary serotonin excretion (C), and HVA excretion (marker of dopamine metabolism) (D). Correlation coefficients are given in Table 2.
Correlations (Spearman) Between Tracer Uptake and Biochemical Activity
DISCUSSION
This study reveals IMT uptake in carcinoid lesions: IMT scintigraphy detected 43% of all lesions and 60% of liver lesions that were positive on 111In-octreotide scintigraphy. Uptake of IMT was lower than uptake of 111In-octreotide, leading to lower lesion contrast and image quality. Interestingly, despite the low detection rate, total IMT uptake was related to the carcinoid biochemical activity, especially to serotonin and dopamine markers. 111In-octreotide uptake correlated with only serotonin metabolism.
How can IMT uptake in carcinoid tumors be explained? In tumor cell lines and in brain tumors, IMT is a substrate for amino acid transport systems, of which the l-transporter for large neutral amino acids is the most important (16,17). Therefore, uptake of IMT in serotonin-producing carcinoids, as found in this study, may be increased because of increased tryptophan transport, resulting in upregulation of the shared amino acid transporter (18). In catecholamine-producing carcinoids, the relation between IMT and dopamine metabolites, which is the first catecholamine in the catecholamine pathway (Fig. 1B), suggests that IMT serves as a false metabolic precursor. An alternative explanation in these latter carcinoids could be binding of IMT to the tyrosine hydroxylase enzyme because the unlabeled compound (methyltyrosine) is known as a catecholamine synthesis-blocking agent through inhibition of this enzyme (27–29). Increased uptake in catecholamine-producing carcinoids cannot be attributed to coexisting serotonin hypersecretion because no correlations were found between markers of serotonin metabolism and catecholamine metabolism (data not shown).
Several reasons may explain the lack of IMT uptake in some carcinoid lesions. First, the uptake of this potential metabolic precursor is probably low in lesions with only minimal secretory activity. This is supported by the positive correlation between IMT uptake and secretory activity. Second, interfering uptake in abdominal organs (kidneys, bladder, intestines) undoubtedly contributes to the negative results (especially in the extrahepatic abdomen). Third, IMT may possibly act a false precursor for catecholamine synthesis, but most carcinoids secrete only limited amounts of catecholamine. This is supported by the higher uptake in dopamine-producing carcinoids in this study and the correlation with the dopamine metabolite excretion. Because both small and large lesions could be negative on IMT images, lesion size apparently does not influence visibility.
Attempts to image carcinoid tumors through a radiolabeled metabolic precursor date back to the late 1960s. Costello (30) showed uptake of [131I]iodotryptophan in human carcinoid tumors using rectilinear scans. Macfarlane et al. (31) published studies using 5-[125I]iodotryptophan, 6-[125I]iodotryptophan, and p-[125I]iodo-dl-phenylalanine, in which tumor uptake was evident in a mouse model. Their subsequent negative studies in 4 patients with carcinoid tumors using p-[131I]iodo-dl-phenylalanine, which had showed the best uptake in mice, were troublesome because of a very low dose, the 131I label, and the use of the racemic mixture instead of the l-isomer. To the best of our knowledge, no other studies using labeled tyrosine (analogs) have been performed in patients with carcinoid tumors. Interestingly, the molecules p-iodo-l-phenylalanine and IMT in the current study are somewhat similar, with the difference being 1 hydroxy group and 1 methyl group.
Since the introduction of receptor imaging with 111In-octreotide, many researchers have lost interest in metabolic targeting of carcinoids. 111In-octreotide scintigraphy is an accurate method to detect metastatic carcinoid lesions with a sensitivity of 80%–90% (8,9,32). This method often detects more lesions than conventional radiologic imaging (8,9). Also, scintigraphy using metaiodobenzylguanidine (MIBG) is a sensitive method to detect carcinoid lesions, although reported sensitivities are lower and results are more variable than for 111In-octreotide (33,34). MIBG is actively transported into the cell and localizes in neurosecretory granules. Whether MIBG preferentially localizes in catecholamine-producing carcinoids is currently unknown but appears logical. Attempts to image carcinoid tumors using FDG were unsuccessful, presumably because of the generally high differentiation grade and low anaerobic glycolysis (35).
A potentially interesting application of labeled metabolic precursors is analysis of therapy-induced changes, for which neither 111In-octreotide receptor imaging nor radiologic imaging has proven very suitable (11–13). Orlefors et al. (36) recently studied the metabolic precursor 5-hydroxytryptophan (5-HTP) labeled with 11C for PET scanning. They found high uptake in multiple carcinoid lesions in 18 patients and observed a close correlation in 5-HTP uptake decrease and 5-HIAA decrease in 10 patients after medical treatment. This finding has revived interest in metabolic imaging of carcinoid tumors. Although our attempt at metabolic imaging with the SPECT tracer IMT is only partly successful, this study shows that many carcinoid lesions take up IMT. One could argue that unlabeled octreotide or interferon might have (negatively) influenced our results because these inhibitors of secretion may decrease the demand for amino acid precursors and could therefore diminish IMT uptake. This cannot be excluded, but, on the other hand, we found no significant difference in IMT uptake between patients on and off secretion-inhibiting medication. It seems most likely that patients on medication have more extensive carcinoid disease, which is also supported by the higher 111In-octreotide uptake despite medication. Furthermore, because lesion sensitivity in patients off medication was no higher than ∼50%, it is unlikely that sensitivity for the whole group would have risen to acceptable levels (80%–100%) only by discontinuing medication.
The relation between total IMT uptake and various secretory products can be of interest, although not directly, for clinical purposes. Identification of catecholamine-producing lesions (among others) could be relevant for selective embolization of these symptom-causing lesions. Clearly, there is a need to search for better tracers in this field that show higher uptake and better lesion contrast. Keeping therapeutic options in mind, the ideal tracer should be selectively localized and trapped in one of the specific metabolic pathways of the carcinoid tumor.
CONCLUSION
The artificial amino acid IMT localizes in many, but not all, carcinoid lesions: IMT scintigraphy detected 43% of all lesions and 60% of liver lesions that were positive on 111In-octreotide scintigraphy. IMT uptake in lesions was lower than 111In-octreotide uptake, leading to lower lesion contrast. Total IMT uptake was related to the carcinoid secretory activity, especially to markers of serotonin and dopamine metabolism. These findings may be of interest in metabolic targeting of carcinoids, especially in catecholamine-secreting tumors, which may lead to development of better tracers to follow the effect of treatment on these tumors.
Acknowledgments
The authors thank Chris Harms, Jelle Boorsma, Annie K. van Zanten, and Gert Luurtsema for performing the IMT syntheses, the technologists for performing and processing all studies, and Rika van der Werff and Bea Vennema for planning studies. The authors are grateful for financial support from Amersham Cygne, Eindhoven, The Netherlands. This work was presented in part at the Society of Nuclear Medicine Annual Meeting, Los Angeles, CA, June 6–10, 1999.
Footnotes
Received Sep. 8, 1999; revision accepted Apr. 4, 2000.
For correspondence contact: Pieter L. Jager, MD, Department of Nuclear Medicine, University Hospital Groningen, P.O. Box 30001, 9700 RB Groningen, The Netherlands.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 111In-Octreotide Is Superior to 123I-Metaiodobenzylguanidine for Scintigraphic Detection of Head and Neck Paragangliomas
- 6-L-18F-Fluorodihydroxyphenylalanine PET in Neuroendocrine Tumors: Basic Aspects and Emerging Clinical Applications
- Radiolabeled Amino Acids: Basic Aspects and Clinical Applications in Oncology