


Abstract
Twenty-eight patients (12 men with prostate cancer, 16 women with breast cancer) were included in a phase II trial to evaluate the efficacy of 186Re-hydroxyethylidene diphosphonate (HEDP) on pain from bone metastasis and the toxicity of this agent. Methods: After intravenous administration of 1295 MBq 186Re-HEDP, the efficacy was evaluated by means of a daily log. Results: We observed an objective response in 67% of prostate cancer patients and in 36% of breast cancer patients. The mean duration of response was 45 d for prostate cancer patients and 24 d for breast cancer patients. No major adverse effects were observed. Marrow toxicity did not exceed grade 2 for white blood cells and grade 3 for platelets using National Cancer Institute criteria. Conclusion: 186Re-HEDP provides safe symptomatic relief of pain in prostate cancer patients. The benefit of this treatment is less clear in breast cancer patients. Further studies should be conducted to evaluate treatment by 186Re-HEDP at an earlier stage of the disease.
Bone metastases are common in patients with primary carcinoma of the breast or prostate (80% of patients with advanced disease have skeletal metastases) (1,2). Seventy-five percent of patients with bone metastases have pain, and 80% of these patients have >1 painful site (3). The longer the evolution, the more bone metastasis develops, compromising the quality of life. Management of pain in patients with bone metastatic disease is a clinical problem. In patients with prostate carcinoma, the response rate to hormone therapy is >70%–85% (4). The duration of response after hormone therapy may be prolonged (average, 12 mo), but relapse with recurrent pain is the rule. In breast carcinoma, only one third of the patients benefit from hormone therapy; when first line hormone therapy has failed, second line treatment is less effective, with a response rate of only 30% (5). Chemotherapy is effective in breast carcinoma but not in prostate carcinoma (4,5). Localized radiation therapy is an effective treatment for patients with solitary or multiple metastasis from either prostate or breast carcinoma. Radiation therapy offers partial or complete relief in 80%–95% of cases (4–6). When there are multiple painful sites, wide-field radiotherapy may be an effective palliative treatment with partial relief of pain in 55%–100% of patients and complete relief in 5%–50%. Toxicity of wide-field radiotherapy may include thrombocytopenia, gastrointestinal symptoms, and pneumonitis. These adverse effects have been reported in up to 30% of treated patients (5,7). Recurrence of pain in other sites may occur in a large number of patients. For many of these patients, the administration of increasing amounts of narcotic analgesics is the only available therapeutic option.
The use of bone-seeking radiopharmaceuticals provides an alternative method of treatment with promising results in terms of pain relief (8–12). Most published studies relate to prostate carcinoma. Few data are available on breast carcinoma. The aim of this study was to evaluate the palliative efficacy and the toxicity of 186Re-hydroxyethylidene diphosphonate (HEDP) in patients with painful bone metastasis of prostate or breast carcinoma.
MATERIALS AND METHODS
Patients
Twenty-eight consecutive patients who were seen over a 2-y period were included in the study. Inclusion criteria were biopsy-proven adenocarcinoma, multiple bone metastases (≥2), failure of prior hormonal therapy or of prior chemotherapy for breast carcinoma, and absence of indication for external radiation. Patients were not included if external radiation was needed for metastasis with pathologic fracture. Exclusion criteria were life expectancy < 3 mo, white blood cell (WBC) counts ≤ 4000 /mm3, total platelet counts ≤ 100,000/mm3, serum creatinine concentration > 133 μmol/L, and performance status according to Karnofsky ≤ 40%. To allow the maximum number of inclusions and taking into account the study of patients with breast carcinoma, the protocol set the lower age limit at 18 y.
Twelve men with prostate carcinoma (average age, 68 y; age range, 60–74 y) and 16 women with breast carcinoma (average age, 59 y; age range, 30–82 y) were included. All patients gave informed consent. Research was approved by the ethical committee of Lille, France.
Tracer Administration
The radiopharmaceutical was administered as a bolus injection through a running intravenous saline drip. Each injection contained 1295 MBq (35 mCi) 186Re-HEDP (Mallinckrodt Medical BV, Petten, The Netherlands).
Post-Therapy Evaluation
All patients were monitored for 3 mo, to the time of administration of external radiation therapy or chemotherapy, or to the time of death. The patients turned in daily logs for the assessment of pain index, analgesic intake, and performance status at each visit (15, 30, 45, and 90 d after the radiopharmaceutical administration). Blood cells counts were performed to evaluate medullary toxicity at each visit.
Clinical therapeutic efficacy was assessed for pain index (1, no pain; 2, mild; 3, moderate; 4, severe; 5, insufferable), analgesic index (graded from 1 to 5 in terms of type of medication and number of doses combined), and performance status (1, easy normal activity; 2, normal activity with effort; 3, need of assistance in daily activity; 4, need of assistance to get out of bed; 5, confinement to bed). Using these indices, different types of objective response were defined. A complete response was characterized as disappearance of pain, with a decrease of analgesic intake together with a stable or improved performance status. The response was considered partial if 1 or more of the 3 criteria showed improvement (but pain did not completely disappear), and none of the others indicated deterioration. The response was considered negative when the 3 criteria were unmodified or when 1 or more worsened.
The subjective response to therapy was also evaluated. This response was based on a single question asked of all patients: “Do you think the treatment is beneficial?”
In addition, bone scanning and skeletal radiography were used to assess changes in the extent of skeletal involvement. Prostate-specific antigen (PSA) or CA 15-3 was measured 6 wk and 3 mo after 186Re-HEDP administration.
The 1988 National Cancer Institute Common Toxicity Scale Criteria were used for the assessment of toxicity (13).
RESULTS
Patients
All patients had received prior external radiation therapy for palliation. Nineteen of the 28 patients were taking narcotics regularly at the time of entry into the study. These treatments failed to decrease pain. Metastatic disease was judged to be extensive on bone scans and standard radiographs (average, 10 bone metastases per patient).
Twenty-three patients underwent a single 186Re-HEDP treatment, 4 received a second treatment, and 1 received a third treatment. Only 26 patients were evaluated. For 2 patients with breast carcinoma, data analysis was not possible because of a lack of information.
Indices of Clinical Efficacy
Pain Index.
Thirty-eight percent (10/26) of patients had a decrease in pain without an increase in analgesic intake (Tables 1 and 2). The pain index decreased by 1 or 2 points (from severe or moderate to mild). A decrease in pain was observed in 50% of patients with prostate carcinoma but in only 29% of patients with breast carcinoma.
Characteristics of Response to Treatment in Prostate Cancer Patients
Characteristics of Response to Treatment in Breast Cancer Patients
Analgesic Index.
Forty-six percent (12/26) of patients had a decrease in their use of analgesic drugs with or without a decrease in pain intensity (7 patients with prostate carcinoma, 5 with breast carcinoma). The analgesic index decreased by 1–4 points (mean, 2 points). In 6 patients, the index was unchanged, and in 8 it increased.
Performance Status.
Six patients had an improvement in performance status. In 14 patients, the performance status was unchanged, and in 6, the score worsened. The performance status showed more variability over time than did the other variables.
No correlation was found between the pain index and analgesic intake and the performance status.
Objective Response
A response was observed between the first and the third week after treatment. The mean duration of response was 47 d for prostate carcinoma and 33 d for breast carcinoma. The percentages of positive responses (complete or partial) after the first injection were 67% for patients with prostate carcinoma (1 complete response, 7 partial responses) and 36% for patients with breast carcinoma (5 partial responses). Two or more criteria were improved in 75% of patients with prostate carcinoma and in 80% of patients with breast carcinoma.
Subjective Response
Eighty-three percent of patients with prostate carcinoma and 50% of patients with breast carcinoma considered the treatment beneficial.
Bone Scans and Biologic Markers
In patients with prostate carcinoma, bone scans were obtained on day 45; only 2 bone scans showed progression of the disease. On day 90, half of the bone scans showed progression. Some lesions became denser on standard radiographs. In patients with breast carcinoma, two thirds of the bone scans showed new hyperfixations on day 45. It was not possible to repeat bone scanning in these patients because of their major deterioration in health or because they had left the protocol (or both).
After therapy, no patient showed a reduction in PSA or CA 15-3 levels. An increase in these markers was observed in 40% of the patients with breast or prostate carcinoma.
Flare Reaction
Eleven (42%) patients experienced a flare reaction (defined by a transient increase in pain intensity after tracer administration). It occurred in the first (n = 8) or second (n = 3) week after the injection and disappeared spontaneously. The intensity of the pain was moderate to severe, and the duration was on average 72 h. No relationship was found between the occurrence of a flare reaction and the response to the treatment.
Toxicity of Treatment
No acute side effects were observed within 30 min after injection. Adverse reactions were observed in 3 patients with breast carcinoma after the 186Re-HEDP injection. On the fifth day, the first patient had an inflammatory ocular reaction with unilateral exophthalmia and edema, together with a supraclavicular tumefaction. These symptoms were short lasting and regressed spontaneously. The second patient presented on the 12th day with a painful inflammation of the left upper palpebra. On the 20th day, pruritis and erythema of the left arm occurred, which was associated with edema and erythema of the right breast. All of these symptoms regressed within 4 d with anti-inflammatory drugs. The third patient had a major episode of high blood pressure with acute heart failure. The patient's condition returned to normal after 30 d of treatment with digitalis and a diuretic.
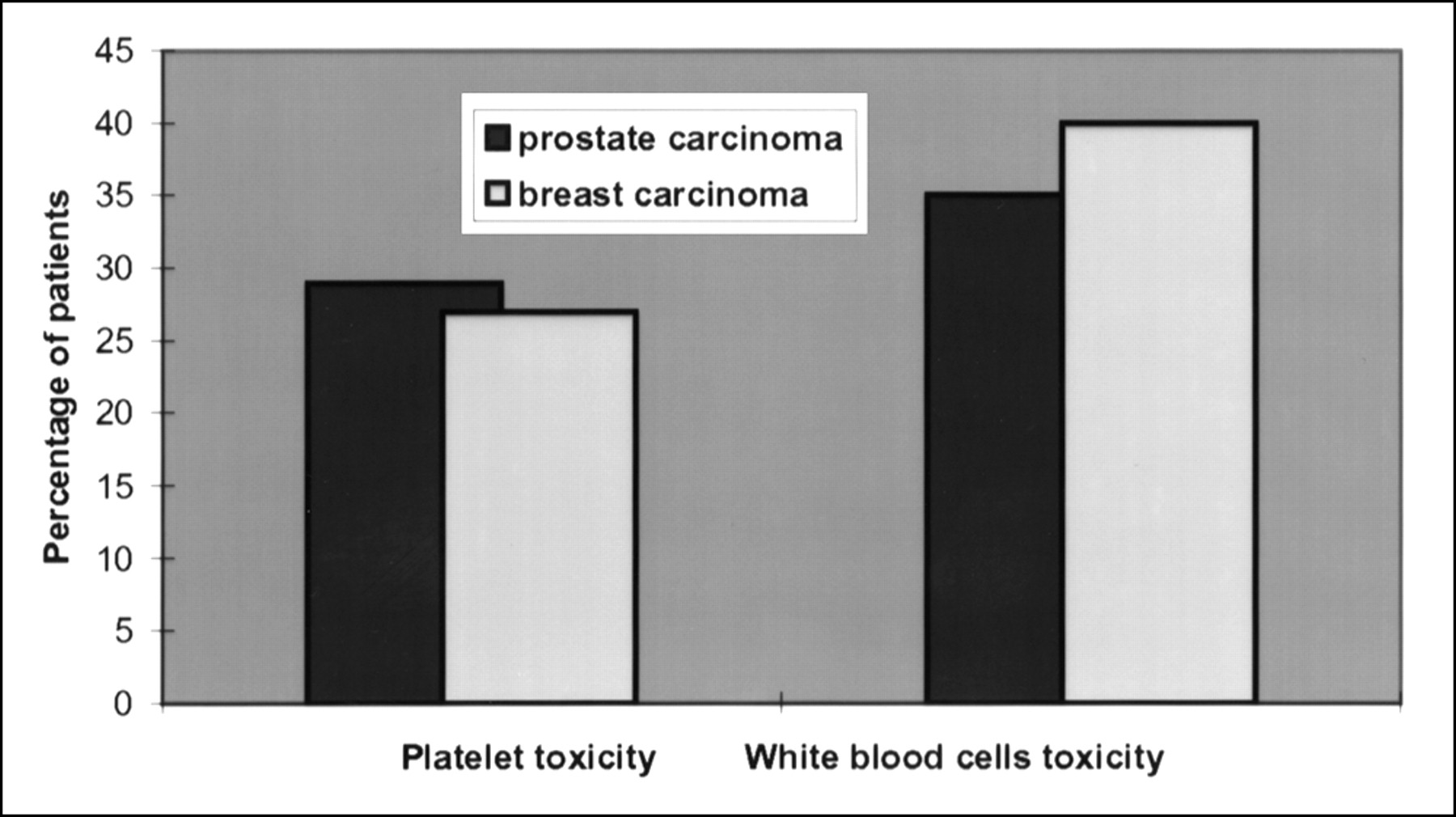
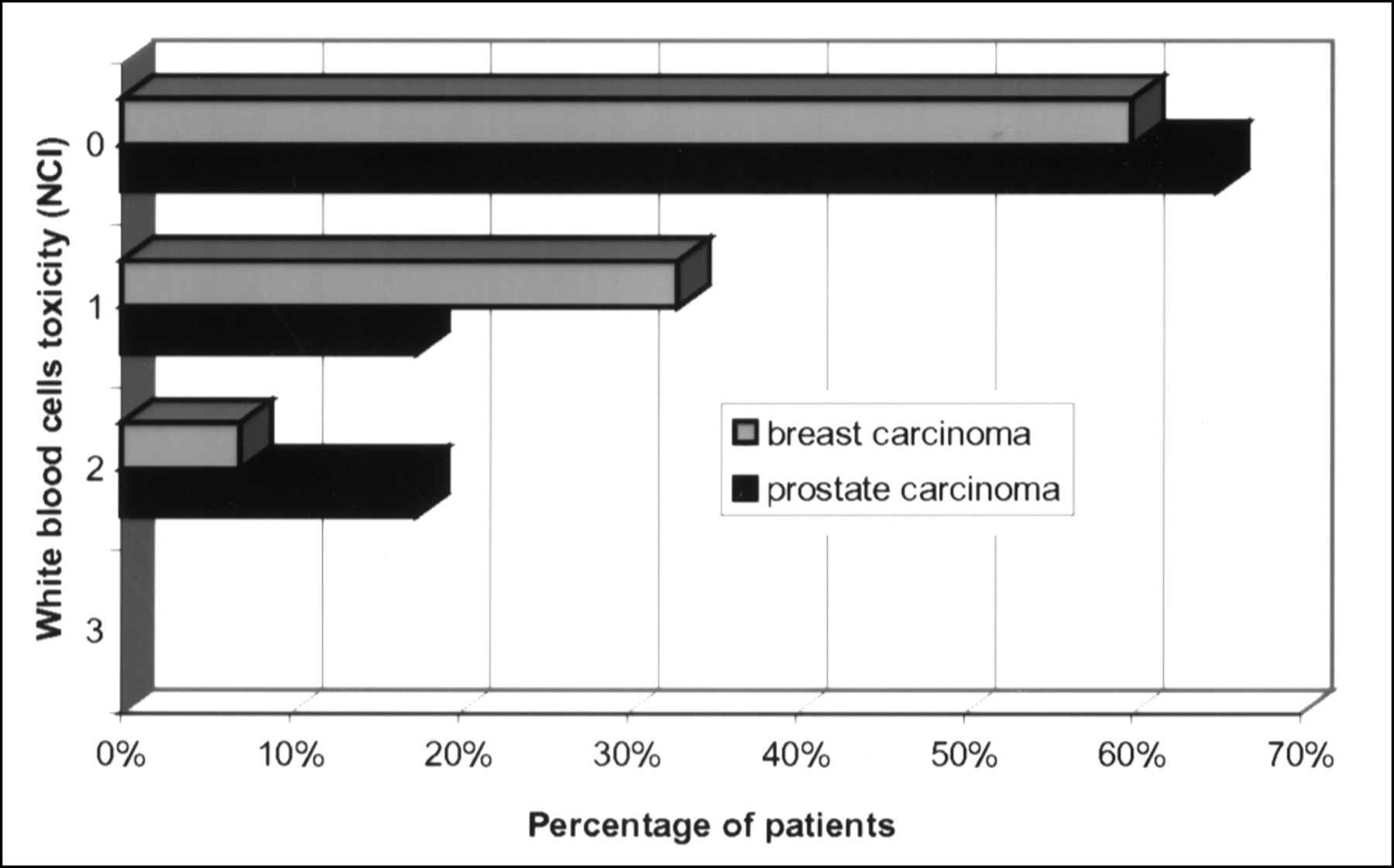
No significant changes occurred over time in the serum creatinine levels of any patient. A decrease in the platelet and WBC counts but no change in the red blood cell count was found. The drop in the WBC count was observed in 35% of the patients with prostate carcinoma and 40% of the patients with breast carcinoma (Fig. 1). The nadir occurred on day 45, with a return to the baseline levels on day 90. Toxicity was moderate (maximum, grade 2) (Table 3). The lowest WBC count was 2600/mm3. The average decreases in WBC counts were 29.5% for patients with prostate carcinoma and 30% for patients with breast carcinoma (Fig. 2).
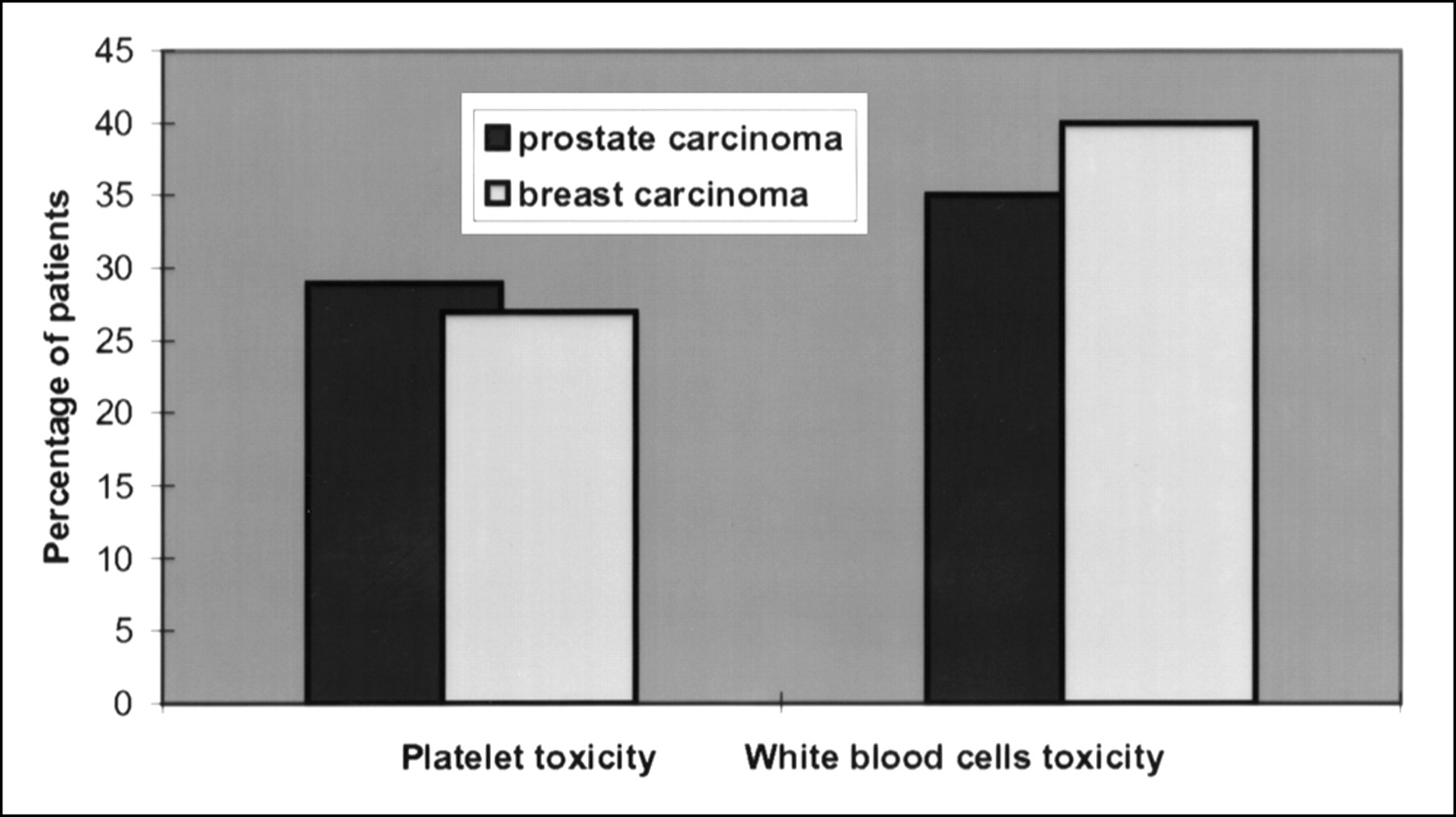
Percentages of patients with platelet and white blood cell toxicity. Note that no more than 40% of patients showed hematologic toxicity.
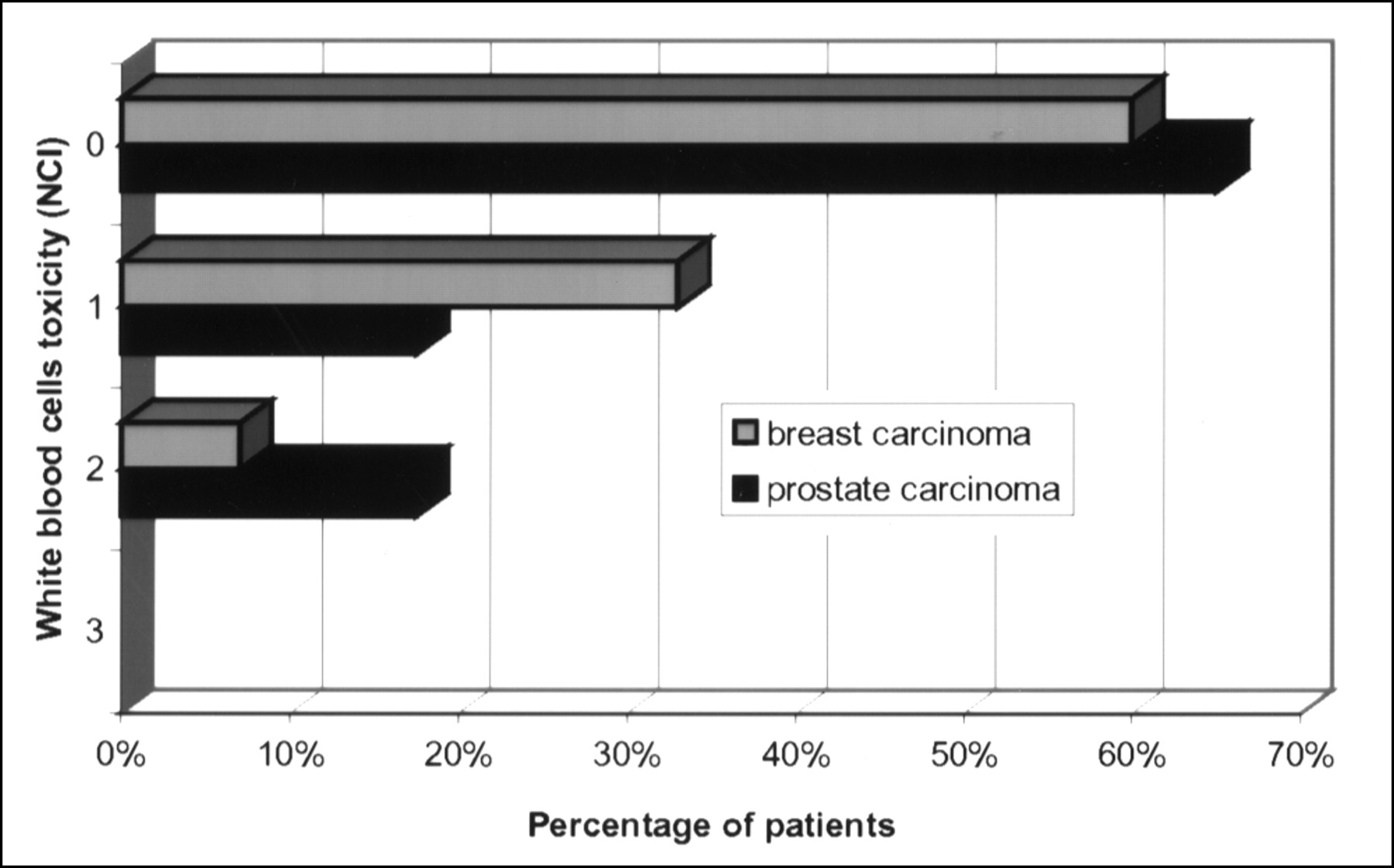
White blood cell toxicity according to National Cancer Institute (NCI) Common Toxicity Scale Criteria (13).
Percentages of Patients with Platelet and WBC Toxicity According to NCI Grading
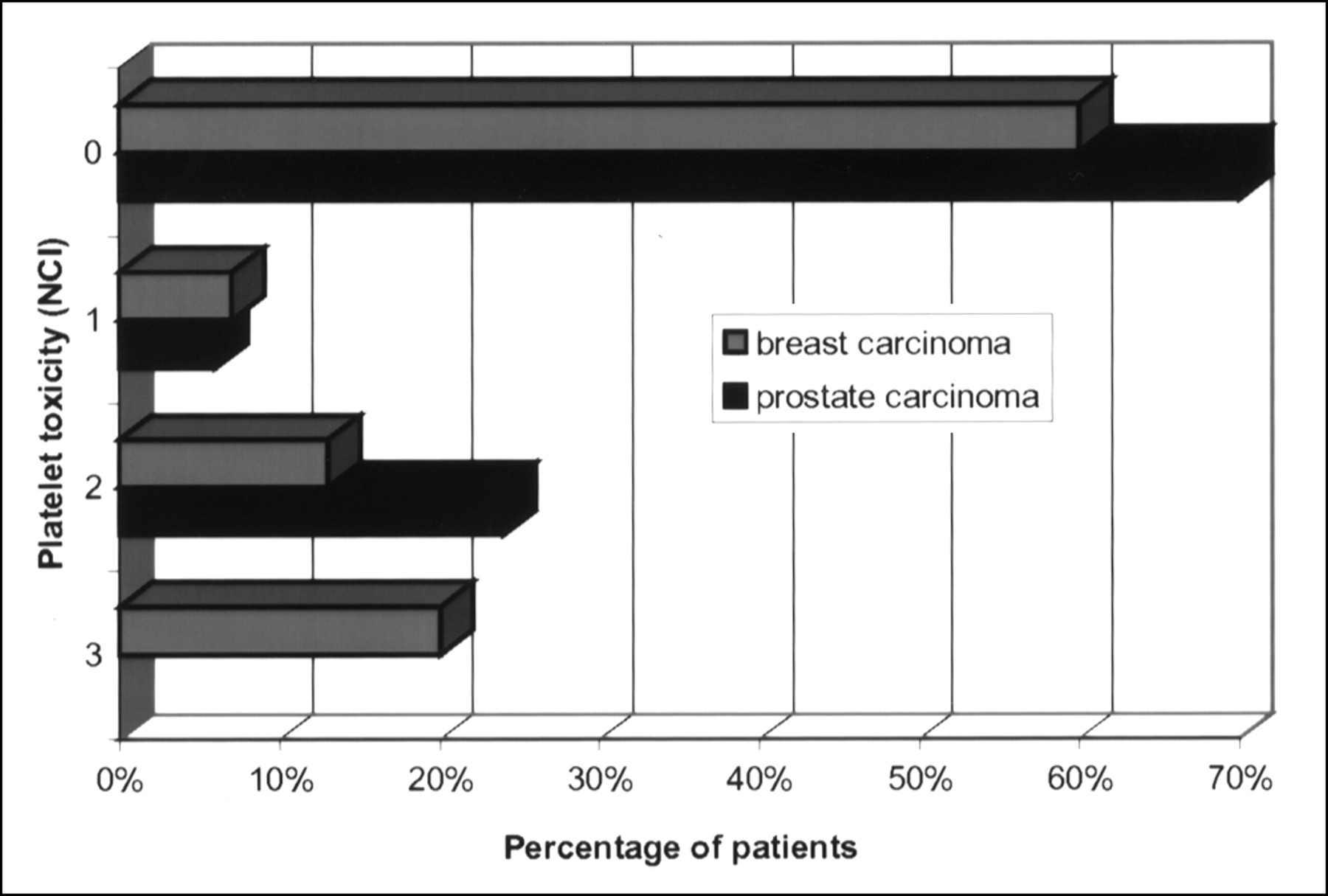
Thrombocytopenia was observed in 29% of the patients with prostate carcinoma and in 27% of the patients with breast carcinoma (Fig. 1). The nadir occurred on day 30, with a return to the baseline levels on day 45. The average decreases in percentages of platelet counts were 37% for patients with prostate carcinoma and 38% for patients with breast carcinoma. Platelet toxicity was confined to grade 2 toxicity for patients with prostate carcinoma; the lowest platelet count was 52,000/mm3. Two patients with breast carcinoma had grade 3 toxicity; the lowest platelet count was 28,000/mm3 (Fig. 3). Nevertheless, the decrease in platelets was not clinically significant and did not contribute to morbidity.
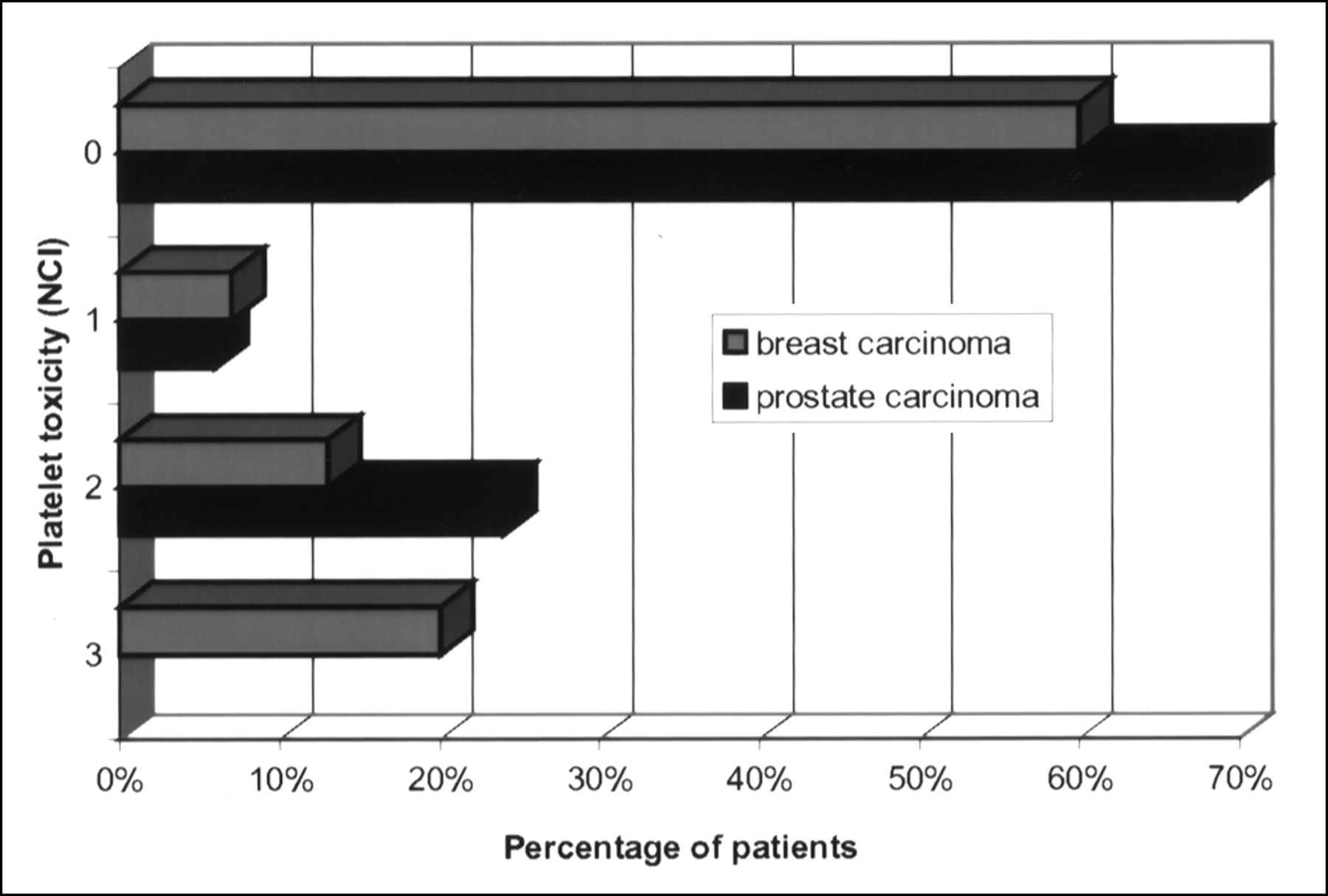
Platelet toxicity according to National Cancer Institute (NCI) Common Toxicity Scale Criteria (13).
Repeated Administrations
Three patients with prostate carcinoma received a second injection of 186Re-HEDP after the objective success of the first injection (between day 56 and day 75). One of the 3 patients received a third injection 5 mo after the second injection because of increasing pain. No objective response (as defined above) to the repeated injections was observed in these 3 patients. There was a stabilization of pain intensity and analgesic treatment. This stabilization lasted 15–35 d after the second injection and 4 mo after the third injection. Two of these 3 patients died at 80 and 120 d after the first injection. Because of additional therapy (external radiation therapy or chemotherapy), it was not possible to repeat the administration of 186Re-HEDP on the other patients who responded to the first treatment.
In 2 other patients (1 with prostate carcinoma, 1 with breast carcinoma), who had only a subjective response after the first treatment, a second dose of 186Re-HEDP was administered. No response (objective or subjective) was observed after the second treatment.
DISCUSSION
All patients in this study were severely ill and had failed traditional treatments. Twenty-five percent of the patients died during this study. Another 25% left the protocol because the acute evolution of their disease required additional treatment (surgery or radiotherapy). Therefore, before the scheduled 90th day, 50% of our patients were no longer included in the study. The average survival of patients after the first 186Re-HEDP administration was 114 d. Only 3 patients were still living after 1 y.
The overall subjective response rate (83% for patients with prostate carcinoma, 50% for patients with breast carcinoma) was similar to published results (9,11,14,15). Most published studies have described only pain assessment, without adjustment for medication index and daily activities. Because of the subjective character of chronic pain, it is difficult to assess the analgesic effect of 186Re-HEDP therapy. With the criteria used in our study, an objective response was observed in 67% of the patients with prostate carcinoma and in 36% of the patients with breast carcinoma. Using similar strict criteria, Quirijnen et al. (11) found a 54% response rate in patients with metastatic prostate carcinoma. However, the difference between the subjective and objective responses cannot be attributed to a placebo effect alone. Maxon et al. (9) reported a significant advantage in pain reduction with 186Re-HEDP treatment compared with placebo responses (subjective improvement after injection was observed in 5 of the 6 patients who received 186Re-HEDP, whereas only 1 of the 7 patients who initially received the placebo injection had such a response). In a study relating to chronic pain in cancer patients who were managed at home (16), 60% of the patients reported in a pain diary that they gained insight into their pain. The use of a pain diary may give patients a sense of control over their pain; as a consequence, the patient's self-administered care may be influenced positively.
The absence of improvement of bone scans and of decrease of blood marker levels shows that, although 186Re-HEDP treatment has an analgesic effect, it does not induce tumor regression.
The difference between the response rates of breast and prostate carcinomas could be explained by the type of bone metastasis. Breast carcinoma typically produces mixed but predominantly lytic lesions in bone, whereas metastases from prostate carcinoma are predominantly osteoblastic. Nevertheless, in our patients with breast carcinoma, no correlation was found between the response rate and the type of bone lesions (lytic or mixed).
The less favorable results in our patients with breast carcinoma may reflect more severely advanced disease (average survival after treatment was 88 d, with no survivors at 7 mo) in comparison with those patients with prostate carcinoma. Life expectancy of the patients is also an important criterion to consider when comparing results between different types of pathologies or different studies.
Even though our patients were elderly, with advanced disease, and had previously undergone extensive therapy that was toxic to the marrow, the changes in the total WBC or platelet counts never exceeded the grade 3 toxicity level, unless additional external radiation therapy or chemotherapy was also given. The decreases were not clinically significant and did not contribute to morbidity. The ability to treat patients who previously had myelotoxic therapies is an important advantage of this form of therapy. Adverse inflammatory reactions in 2 patients could be attributed to the β radiation. Deficits in cranial nerves secondary to edema around skull bone metastases have been reported (17).
Studies have shown the efficacy of repeated administration, particularly if the patient responded to the first treatment (9,14,17,18). In our study, the 5 patients who received repeated sequential treatment with 186Re-HEDP had stabilization of pain without an increase of narcotic intake. Contrary to results in the literature, we did not find that repeated 186Re-HEDP administration gave positive objective results as defined above.
CONCLUSION
Our clinical data prove that 186Re-HEDP can provide safe, symptomatic relief of painful metastasis in prostate cancer patients. The opportunity of treating multiple painful metastatic sites is a clear advantage of this agent. Its effects on metastatic breast carcinoma are less convincing; therefore, it would be of interest to test its efficacy earlier in the course of this disease.
Acknowledgments
The authors thank Professor Michel Meignan, Doctor Charles Bruneau, and Micheline Levame for their wise advice. This investigation was supported by Mallinckrodt Medical BV, Petten, The Netherlands.
Footnotes
Received Oct. 19, 1999; revision accepted Feb. 16, 2000.
For correspondence or reprint requests contact: Charles Sulman, MD, Department of Nuclear Medicine, Centre Oscar-Lambret, 1 rue Frederic Combemale, 59000 Lille, France.




{kind=link}
{kind=link}
{kind=link}