


Abstract
Variable success rates for identifying axillary (AX) sentinel nodes in breast cancer patients using preoperative lymphoscintigraphy have been reported. We evaluated the effects of age, weight, breast size, method of biopsy, interval after biopsy, and imaging view on the success of sentinel node identification and on the kinetics of radiopharmaceutical migration. Methods: Preoperative breast lymphoscintigraphy was performed in consecutive breast cancer patients from February 1998 to December 1998. The ipsilateral shoulder was elevated on a foam wedge and the arm was abducted and elevated overhead. Imaging using this modified oblique view of the axilla (MOVA) started immediately after peritumoral injection of Millipore-filtered 99mTc-sulfur colloid and continued until AX sentinel nodes were identified. Anterior views were obtained after MOVA. AX, internal mammary (IM), and clavicular (CL) basins were monitored in all patients. MOVA was compared with the anterior view for sentinel node identification. Age, weight, breast size, method of biopsy, interval after biopsy, and primary tumor location were evaluated for their effects on sentinel node localization and transit times from injection to arrival at the sentinel nodes. Results: Seventy-six lymphoscintigrams were obtained for 75 patients. AX sentinel nodes were revealed in 75 (99%) cases. IM or CL sentinel nodes were found in 19 (25%) cases and were not related to tumor location; exclusive IM drainage was present in 1 (1%) case. Identification of AX sentinel nodes was equivalent with MOVA and anterior views in 18 (24%) patients, was better with MOVA in 20 (26%) patients, and was accomplished only with MOVA in 38 (50%) patients. Median transit time was 17.5 min (range, 1 min to 18 h) after injection, and larger breast size was associated with increased transit time. No effect of age, weight, biopsy method, interval from biopsy, or tumor location on transit time was found. Conclusion: Use of MOVA can improve identification of AX sentinel nodes. Although AX drainage is the predominant pattern, a tumor in any portion of the breast can drain to IM sentinel nodes. Transit time was influenced by breast size. Overall short arrival times with this technique allow sentinel lymph node dissection to be performed on the same day as lymphoscintigraphy.
Sentinel lymph node dissection (SLND) is a minimally invasive method for staging patients with breast cancer. The technique uses an agent, either a vital dye or a radiopharmaceutical, that enters the lymphatics of the breast after peritumoral injection and concentrates first in 1 or 2 regional nodes, the sentinel nodes. Because these initial nodes encountered by lymph draining from a primary breast tumor are the most likely sites of any regional nodal metastases, they are excised and examined as an indicator of nodal status. The sentinel node concept was popularized by Morton et al. (1) in melanoma and extended to breast cancer by Krag et al. (2) and Giuliano et al. (3,4). Preoperative lymphoscintigraphy of the breast has frequently accompanied SLND in many centers as an adjunct to intraoperative localization. It reveals drainage from the primary tumor to the axillary (AX), internal mammary (IM), or clavicular (CL) sentinel node(s) and provides a focused approach to subsequent radioguided surgery using an intraoperative γ probe to identify the sentinel node (5–12).
Although the techniques used for preoperative lymphoscintigraphy are highly variable, successful identification of sentinel nodes is between 75% and 98% (7–12). Geometric and other factors affecting kinetics of radiopharmaceutical migration and success of sentinel node identification have not been extensively studied, particularly the effect of patient position when imaging is undertaken after recent biopsy. Therefore, we evaluated the effect of a change in patient position to obtain a modified oblique view of the axilla (MOVA) and compared this with a standard anterior view of the supine patient for identification of AX sentinel nodes. Second, we examined the effects of age, weight, breast size, method of biopsy, and interval from biopsy to lymphoscintigraphy on the rate of sentinel node identification and the transit time of the radiopharmaceutical. Patterns of lymphatic drainage were correlated with tumor location.
MATERIALS AND METHODS
Patients
Candidates for this study were all consecutive female patients with a cytologic or tissue diagnosis of invasive breast carcinoma, who underwent breast lymphoscintigraphy before SLND from February 1998 to December 1998.
Lymphoscintigraphy
Preoperative breast lymphoscintigraphy was performed after preparing the skin with alcohol and using 2 mL 1% xylocaine for local anesthesia. A total of 12–16 MBq 99mTc-sulfur colloid (CisUS, Bedford, MA), passed through a 200-nm Millipore filter (Millipore Corp., Bedford, MA) in a total volume of 3–8 mL, was injected around the tumor or in the wall of the biopsy cavity. The volume injected varied with the size of the breast. Injections were not performed into biopsy cavities or seromas.
Planar images of the breast, axilla, supraclavicular, and infraclavicular regions were acquired using a scintillation camera with acquisition times that allowed adequate visualization of the lymphatic drainage basin. Usual acquisition times varied from 1 to 5 min. MOVA images were obtained after elevating the ipsilateral shoulder to 45° on a triangular foam wedge and raising the arm overhead. Imaging began immediately after injection and continued sequentially until sentinel nodes were identified. After the AX sentinel nodes were identified, a handheld γ probe was used to confirm the location of the nodes. The skin was marked on the basis of confirmation of image localization by the handheld γ probe. If sentinel nodes were not identified by 4–6 h, the patient was brought back for imaging the next day. Transit times from injection to sentinel node identification were recorded. AX, IM, and CL basins were monitored in all patients to determine primary and secondary drainage. Once the AX sentinel nodes were localized and marked on the skin, the patient was moved to the supine position and imaged in the anterior projection using the same acquisition times. Anterior supine and MOVA images were compared for success in identification of sentinel nodes.
SLND
All patients underwent AX SLND either the same day or 1 d after breast lymphoscintigraphy. No patient underwent IM or CL SLND. SLND was performed using vital dye or a handheld γ probe (or both). The specific technique was chosen at the discretion of the attending surgeon. For the studies performed with vital dye, 3–5 mL isosulfan blue (Lymphazurin 1%, U.S. Surgical Corp., Norwalk, CT) were injected into the breast parenchyma adjacent to the primary tumor or into the wall of the biopsy cavity if a previous excision had been made. Through a separate axillary incision, a blue lymphatic was dissected and traced to blue sentinel nodes, which were excised. After SLND, the primary tumor was removed during total mastectomy or lumpectomy. A complete axillary lymph node dissection was performed only in patients whose sentinel nodes were positive for metastases.
For the studies performed using radioguided surgery with a γ probe, an incision was placed over the hot spot in the axilla, and, using the probe as a guide, radioactive sentinel nodes were removed until counting rates dropped to background level. Some studies were performed using a combination of the 2 techniques. Because not all dissections were performed using both techniques, we did not correlate blue sentinel nodes with radioactive sentinel nodes.
Sentinel nodes were bivalved and submitted for frozen or permanent section. Frozen tissue was processed routinely for permanent section using hematoxylin and eosin staining. Sentinel nodes were submitted in separate cassettes for paraffin embedding. If metastases were not identified using hematoxylin and eosin, immunohistochemistry was performed using anticytokeratin antibodies (MAK-6; Ciba-Corning, Alameda, CA). Six to 8 sections were examined from each sentinel node.
Data Analysis
The 2 primary outcome measures were AX sentinel node identification rate by lymphoscintigraphy using the 2 imaging views and transit time of the radiopharmaceutical to the sentinel node after injection. The secondary outcome measures were the location of the sentinel nodes in the AX, IM, or CL drainage basins. The 2 primary outcome measures were assessed with respect to 6 factors: age, weight, breast size, injection quadrant, interval from biopsy to lymphoscintigraphy, and method of biopsy. Breast size was determined subjectively by the same 2 technologists for each case and was designated as small, medium, or large.
Statistical Analysis
The outcomes for comparing sentinel node identification from the 2 images were classified as MOVA equivalent to the anterior view, MOVA superior to the anterior view, or seen only with MOVA. Logistic regression was used to assess the effect of each of the 6 factors on sentinel node identification using MOVA and the anterior view. A nonparametric permutation test on the linear model was performed to determine the effect of the 6 factors on radiopharmaceutical transit time. A normality test showed that transit time was not distributed normally. Fisher's exact test was used to analyze the association between injection quadrant and sentinel node location. All Ps were 2-tailed, and an α level of 0.05 was considered significant.
RESULTS
Of the 75 patients (median age, 59 y; age range, 29–81 y) identified in the study period, 1 had synchronous bilateral breast cancer and underwent staged bilateral lymphoscintigraphy and SLND. Thus, 76 localization studies were analyzed. Most patients had invasive ductal carcinoma (Table 1). All patients underwent fine-needle aspiration, needle core biopsy, or excisional biopsy for diagnosis a median of 14 d before lymphoscintigraphy. Patient weight ranged from 45 to 107 kg, with a median of 63 kg. Breast size was small in 21 patients, medium in 32 patients, and large in 22 patients. There were 38 (50%) lesions in the inner quadrants and 37 (49%) in the outer quadrants; 1 patient (1%) had a tumor in the subareolar area.
Patient Demographics and Tumor Characteristics
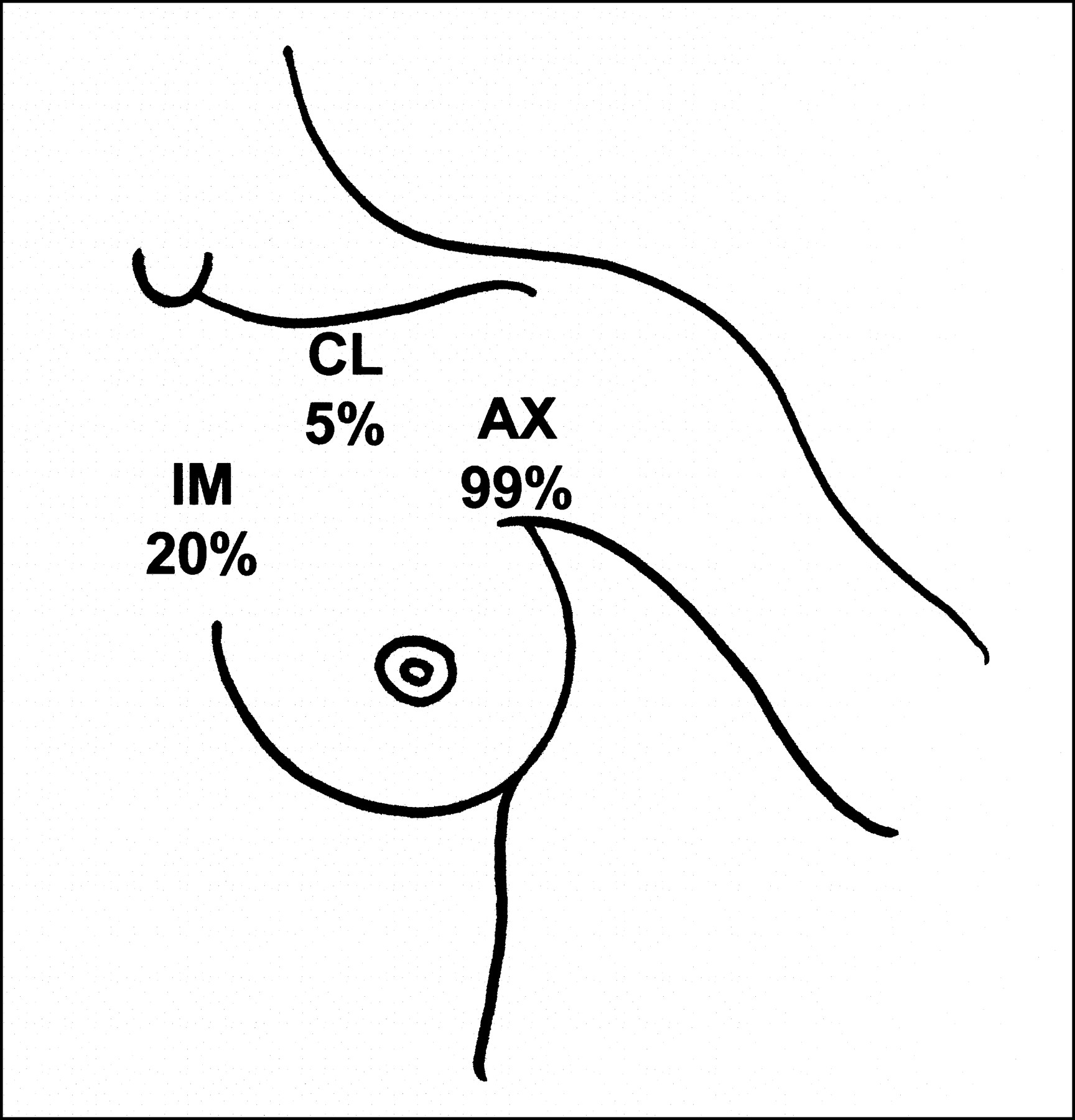
Overall, the 76 lymphoscintigrams revealed 75 (99%) AX drainage basins, 15 (20%) IM drainage basins, and 4 (5%) CL drainage basins (Fig. 1). Individual drainage patterns are summarized in Table 2. In 59 cases, the lymphoscintigrams identified a single primary drainage basin (58 AX and 1 IM). In 2 cases, lymph drained equally to separate primary nodal basins (AX + IM and AX + IM + CL). In 15 cases, lymph drained unequally to primary and secondary basins (8 AX > IM, 4 IM > AX, 2 AX > CL, and 1 CL > AX). Primary AX or IM sentinel node location was not dependent on the primary tumor location; sentinel nodes were located in AX nodes in 92% and in IM nodes in 5% of inner quadrant lesions compared with 92% AX and 8% IM sentinel nodes of outer quadrant lesions (P = 1.0).
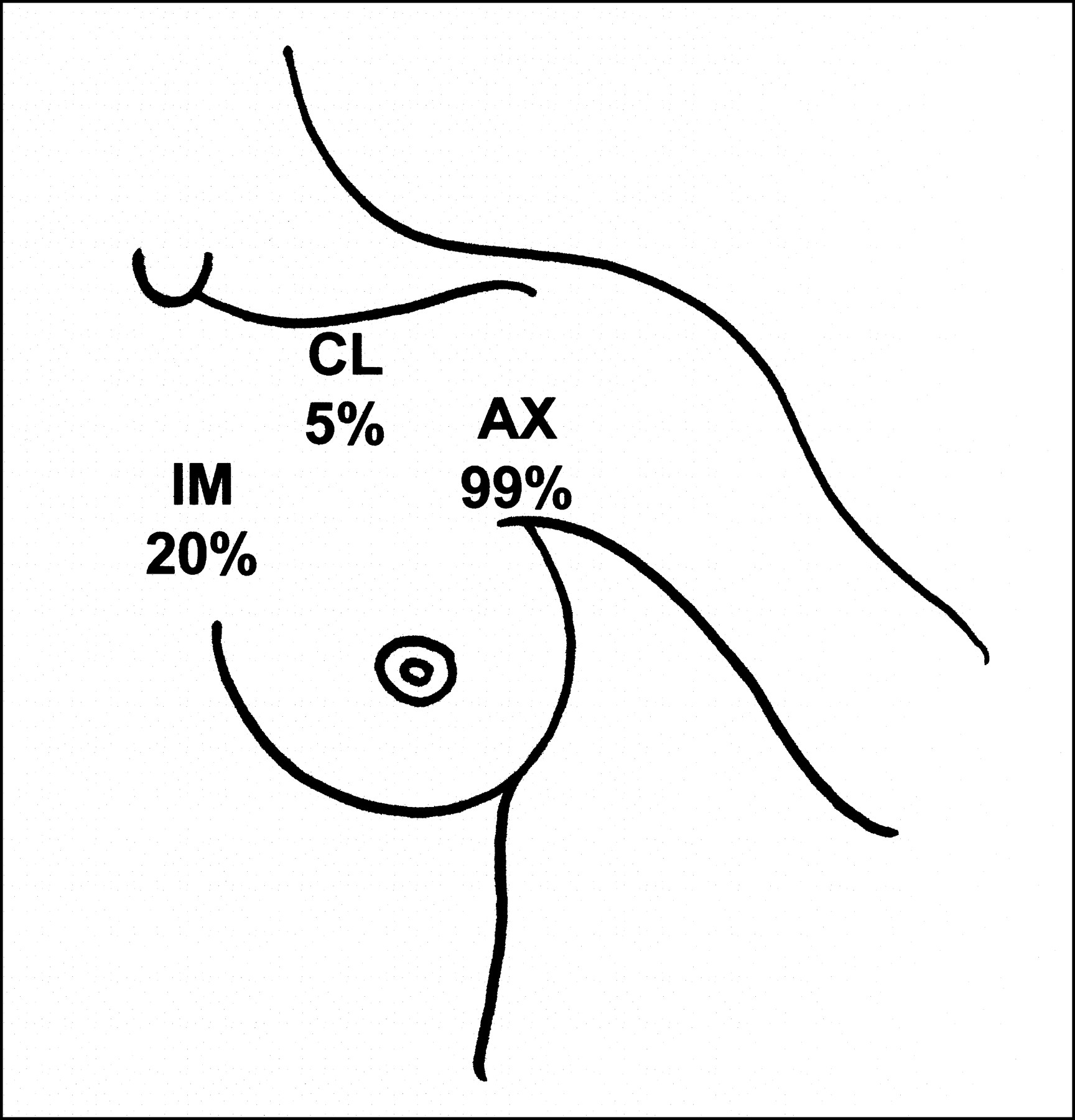
Frequency of AX, IM, and CL sentinel nodes found on preoperative lymphoscintigraphy in all cases. No correlation was found between inner versus outer quadrant primary tumors and location of sentinel node.
Primary and Secondary Drainage Patterns in 76 Breast Lymphoscintigrams
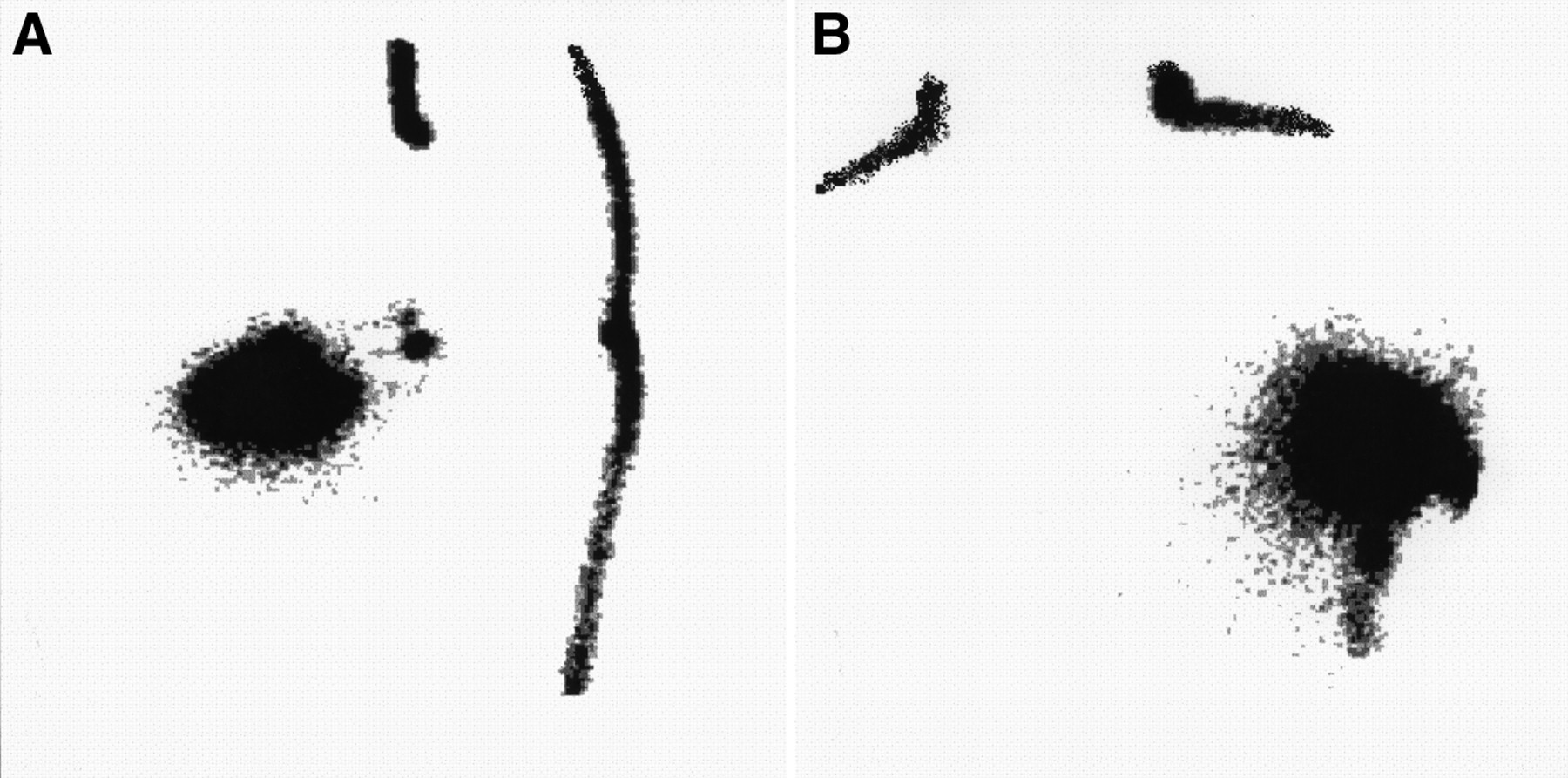
When results of MOVA and anterior views were compared, the detection of AX sentinel nodes was equivalent in 18 cases, superior with MOVA in 20 cases, and possible only with MOVA in 38 cases. Therefore, MOVA identified 100% of AX sentinel nodes, whereas the anterior view identified only 50% (P < 0.001). AX sentinel nodes depicted in MOVA but not seen in the anterior view in the same patient are illustrated in Figure 2. The injection quadrant, whether inner or outer, had no effect on whether AX sentinel nodes were detected exclusively or more effectively with MOVA compared with AX sentinel nodes that were detected equally by MOVA and the anterior view (P = 0.45).
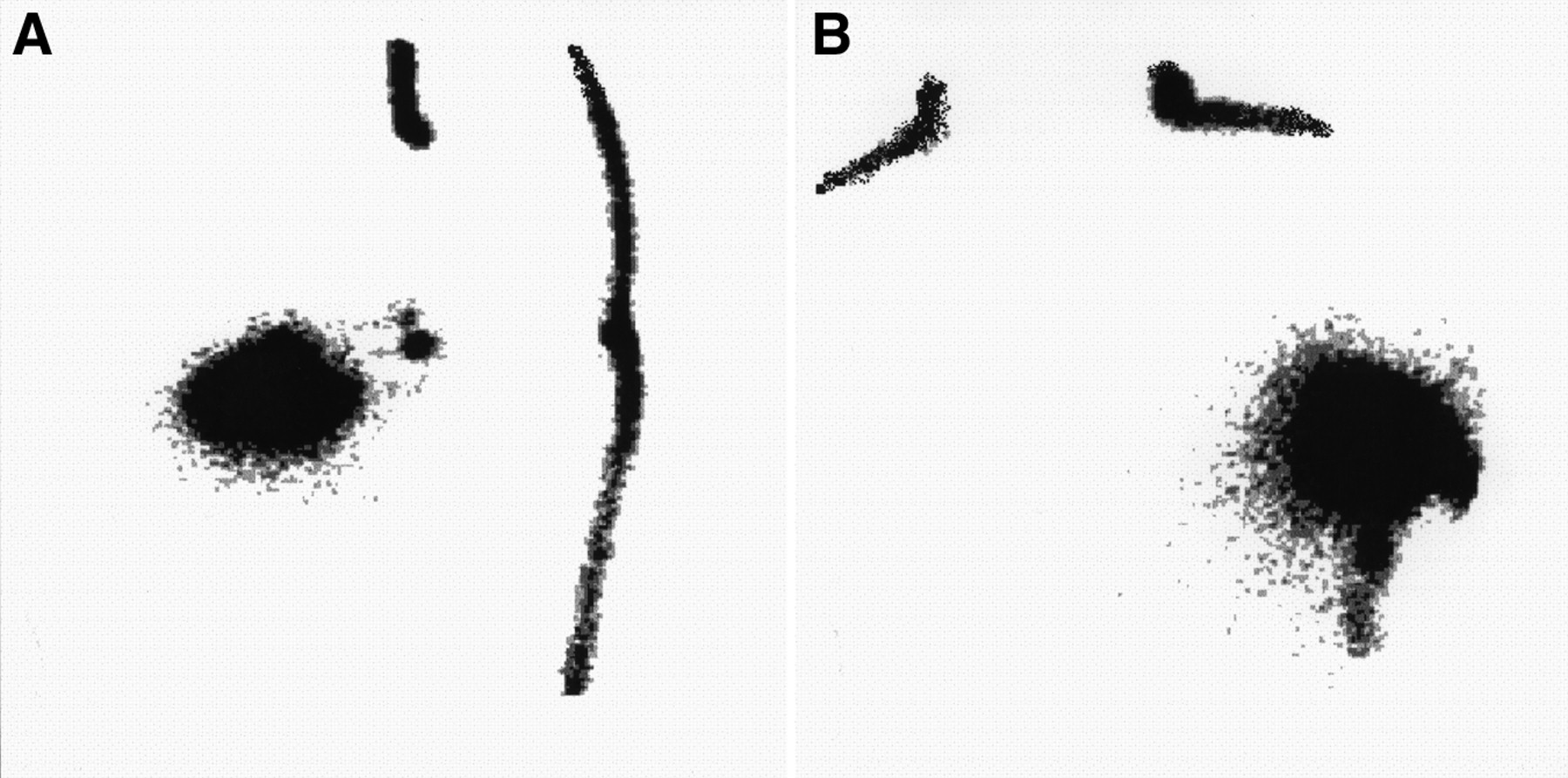
Lymphoscintigrams from patient with upper outer quadrant tumor in left breast 30 min after injection at primary tumor site. MOVA shows distinct AX sentinel nodes (A) that are not seen on anterior view (B). MOVA revealed AX sentinel nodes in all patients, whereas anterior view missed 50% of AX sentinel nodes.
After injection, transit time of the radiopharmaceutical to the sentinel node ranged from 1 to 1080 min, with a median of 17.5 min. Median transit times were 92 min for large breasts, 26 min for medium breasts, and 23 min for small breasts. No effect of age, weight, biopsy method, or biopsy interval on transit time was identified (Table 3).
Effect of 6 Factors on Radiopharmaceutical Transit Time Determined by Logistic Regression
SLND was performed in 37 cases on the same day and in 39 cases on the day after lymphoscintigraphy. AX sentinel nodes were identified during surgery in all patients. Metastases were present in 28 (37%) patients (Table 4). Twenty (71%) of the patients with sentinel node metastases had micrometastases (<2 mm); in 8 patients, these micrometastases were limited to occasional scattered cells detectable only by immunohistochemistry. In 2 patients who had dominant IM drainage and secondary AX drainage, metastases were present in the AX sentinel node. In the 1 patient who had dominant CL drainage and secondary AX drainage, metastases were present in the AX sentinel node.
Pathology of Sentinel Nodes
DISCUSSION
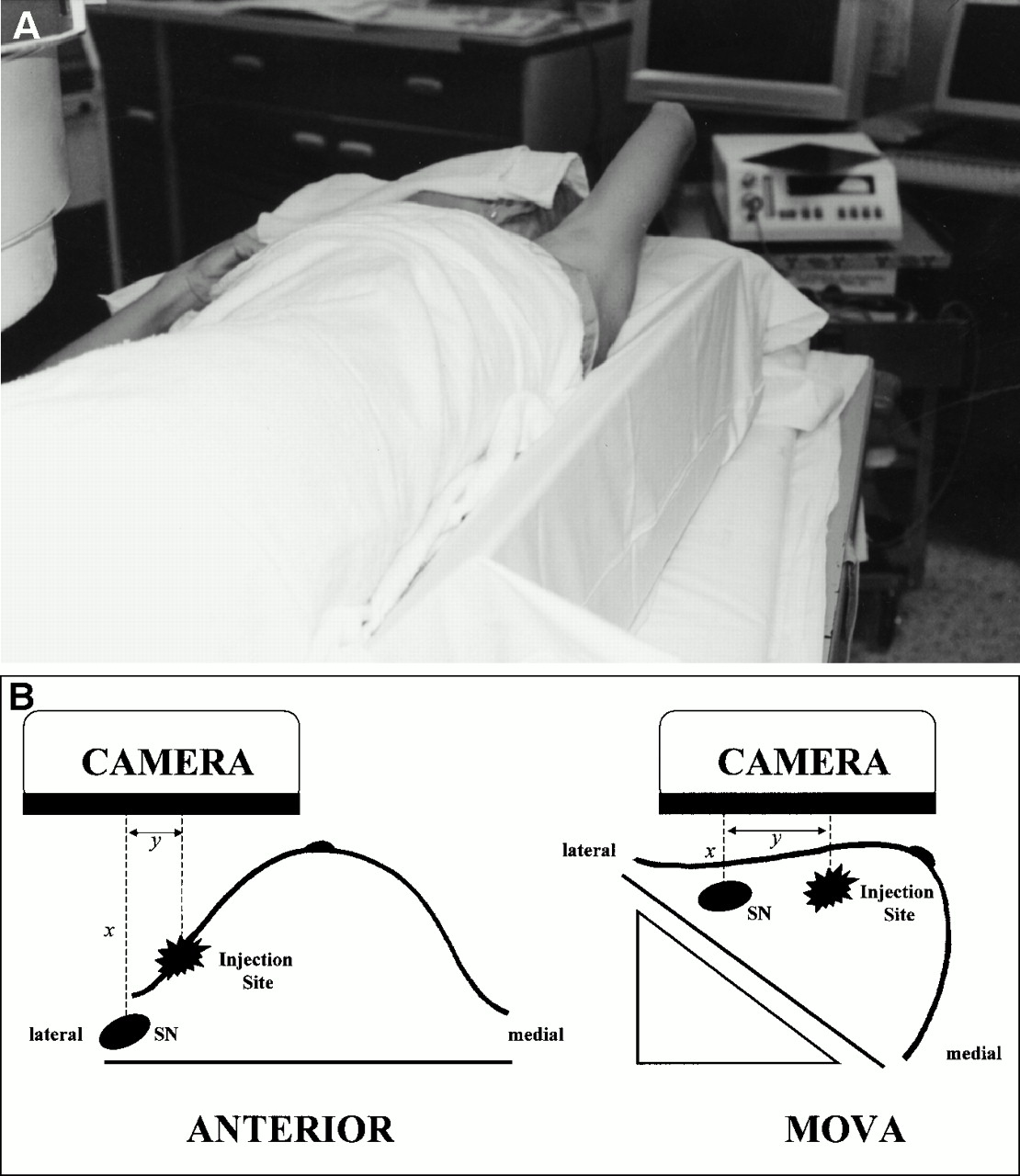
Lymphoscintigraphy localized a sentinel node in all cases. Imaging with MOVA frequently identified AX sentinel nodes not imaged with the anterior projection. Positioning the patient in the supine position with the arm abducted and elevated overhead separates the radioactive injection site from the less radioactive sentinel node, facilitating identification of the sentinel node (Fig. 3). MOVA is equally effective for tumors in inner and outer quadrants. This is in agreement with the results of De Cicco et al. (9), which documented the necessity of oblique views for determining the skin projection of the AX sentinel node. However, the anterior view is still required to image the IM nodes (Fig. 4). The usefulness of MOVA is related to geometric factors. In MOVA the sentinel node is closer to the scintillation camera, which improves sensitivity (Fig. 3), and activity from the injection site is less likely to overlap the sentinel node. As the shoulder is elevated, gravitational translation of the breast away from the axilla provides better separation of the intense activity in the injection site from the less-intense activity in the sentinel node. An added advantage is that this position approximates most accurately the position of the patient's arm during surgery, which facilitates sentinel node identification and removal.
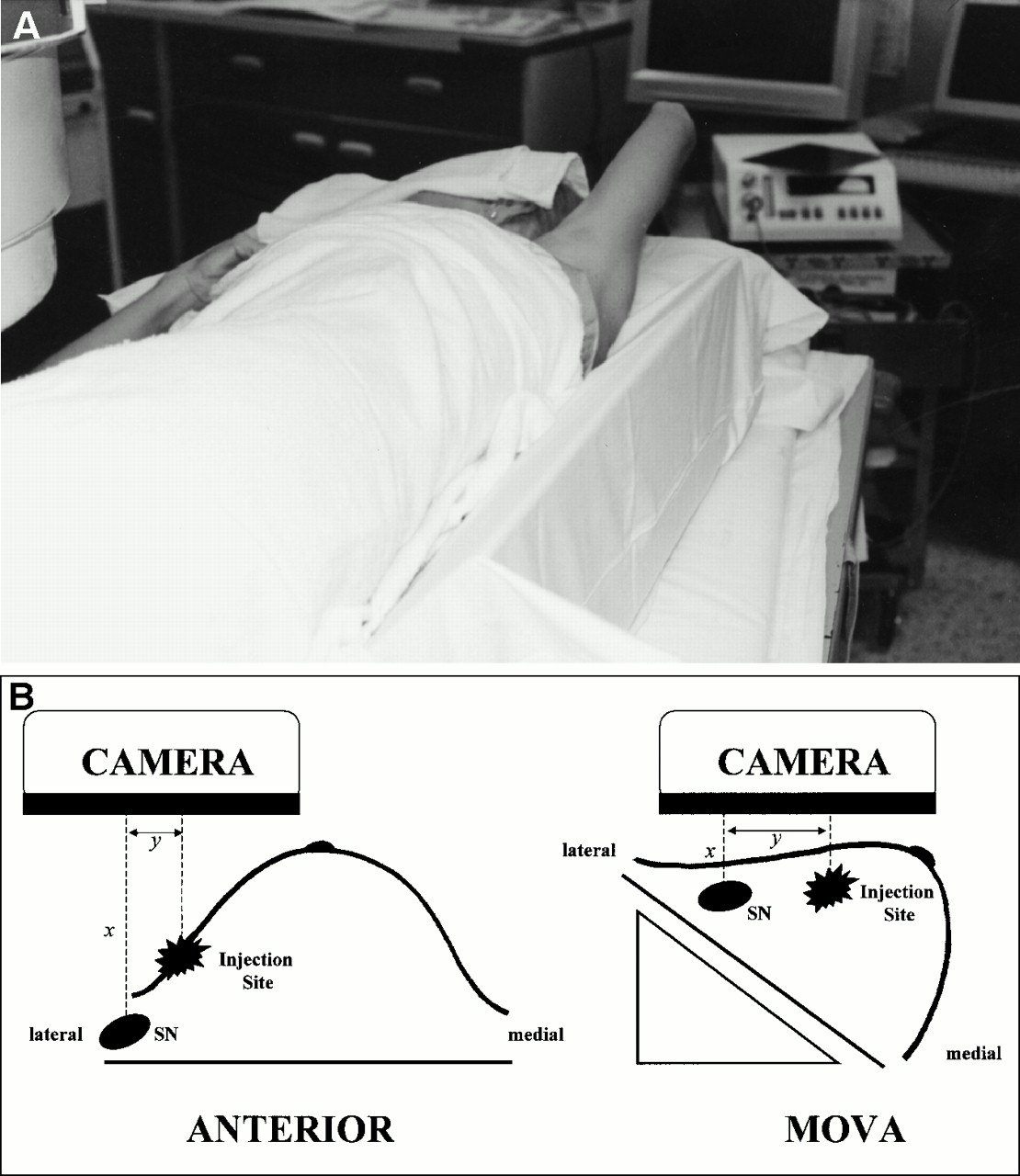
(A) Patient positioned on foam wedge with arm extended and abducted overhead to obtain MOVA image. (B) Schematic representation of craniocaudal view of breast at time of lymphoscintigraphy for outer quadrant tumor. (Left) In anterior view, distance projected onto scintillation camera (y) from injection site to AX sentinel node (SN) is short. (Right) Using MOVA, patient positioning on 45° wedge allows breast and injection site to shift medially from AX sentinel node, increasing distance y, and brings sentinel node closer to gamma camera (x), thereby improving AX sentinel node identification.
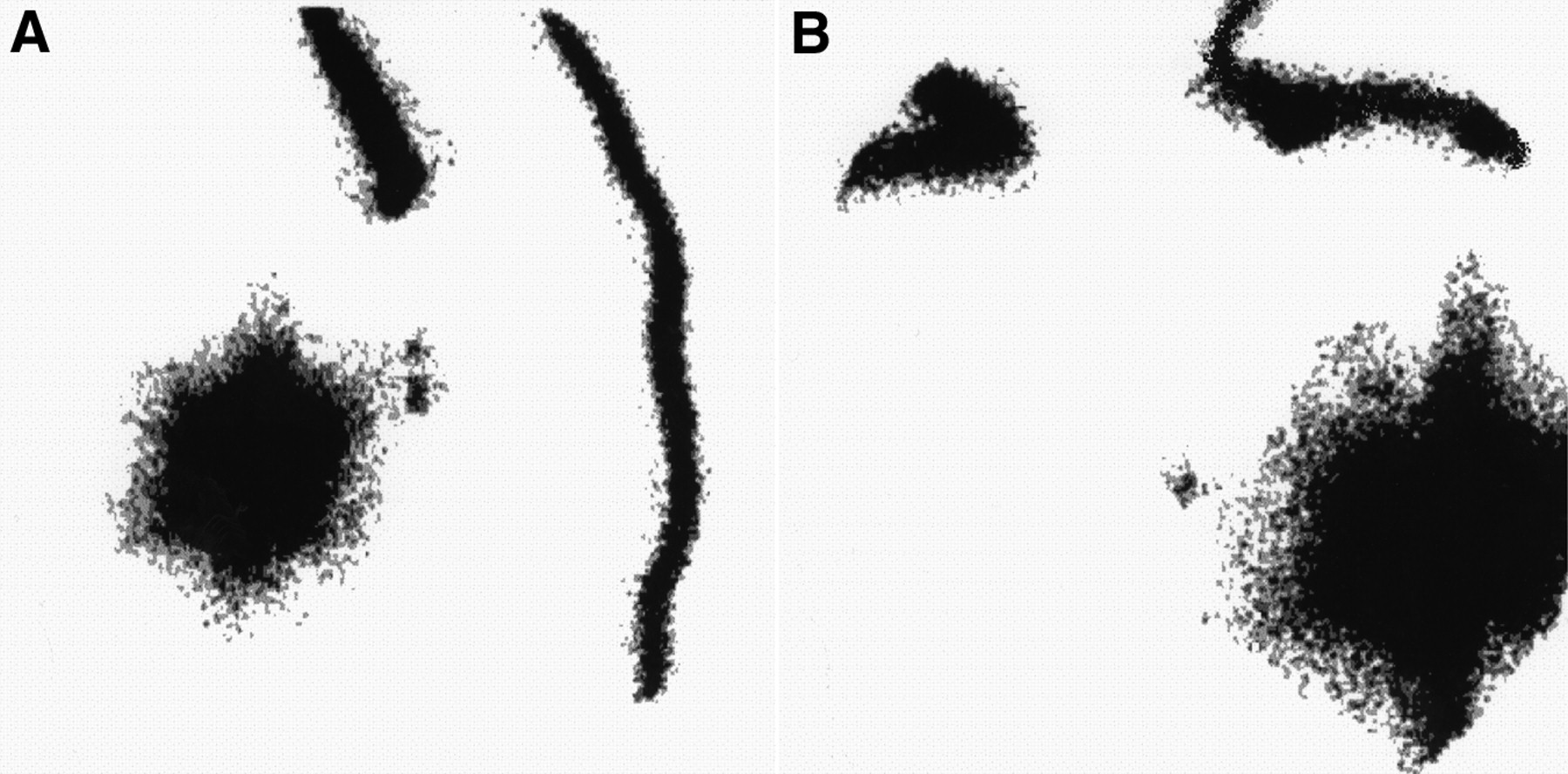
Lymphoscintigrams from patient with upper outer quadrant tumor in left breast 15 min after injection at primary tumor site. MOVA reveals AX sentinel nodes (A), whereas anterior view shows distinct IM sentinel node, but AX sentinel nodes are not visualized (B). Both MOVA and anterior images must be obtained to evaluate all regional drainage sites.
The radiopharmaceutical transit time to the sentinel node was slower in women with large breasts than in women with smaller breasts. However, the transit time even in patients with larger breasts remains reasonable, so that lymphoscintigraphy performed early in the morning can be followed by SLND in the afternoon. Thus, axillary staging can be consolidated into a single day.
All but 1 patient had lymphoscintigraphy showing some AX drainage. Only 7 of 76 studies revealed dominant IM drainage. These migration patterns are consistent with other reports of lymphoscintigraphy before SLND (Table 5). Migration to non-AX sites was not predictable by the quadrant of the breast injected. Other studies have shown that IM drainage can occur with both inner and outer quadrant lesions (7,12).IM drainage is usually accompanied by AX drainage. The 1 patient with exclusive IM drainage on lymphoscintigraphy had a blue-stained AX sentinel node visualized during SLND. In many cases, the 2 methods for identifying the sentinel node are complementary, and the dye or radiopharmaceutical will aid in sentinel node detection when the other method fails (8–11).
Summary of Techniques and Drainage Patterns in SLND Series Using Breast Lymphoscintigraphy
Many investigators do not obtain lymphoscintigrams after injection and rely solely on intraoperative localization with a handheld γ probe (13–15). After injection of the radiopharmaceutical, the patient is taken to the operating room; then, usually with the patient under general anesthesia, hot spots are marked on the skin using the γ probe. The time spent searching for hot spots with the probe is likely equal to that of lymphoscintigraphy. However, lymphoscintigraphy also documents drainage to all lymph node areas and more easily identifies failed radiopharmaceutical migration. If hot spots are not identified with the probe, then reasons other than migration failure, such as probe malfunction, may be responsible for failed sentinel node detection; this can be difficult to appreciate without a preoperative lymphoscintigram. Similarly, a hot spot found with the γ probe may originate from radiopharmaceutical that has leaked onto the skin; this would be obvious on lymphoscintigraphy but more difficult to deduce with a probe. This may be 1 reason why sentinel nodes were not always detected beneath the skin hot spots in the multicenter trial reported by Krag et al. (13). In the same trial, all false-negative findings occurred with primary lesions that were in close proximity to the axilla. Lymphoscintigraphy using MOVA can aid in identifying nodes that are close to the injection site, a difficult distinction when the probe alone is used—particularly if the patient is kept supine during probe localization, as in the multicenter trial. Finally, it is uncommon for the γ probe alone to identify a radioactive sentinel node that was not localized by lymphoscintigraphy (6,9). When multiple nodes are hot, the probe alone cannot reliably distinguish sentinel from nonsentinel nodes, whereas dynamic lymphoscintigraphy easily permits this distinction. Therefore, preoperative lymphoscintigraphy will usually reveal the sentinel node before radioguided surgery, making it unnecessary to remap drainage sites intraoperatively with the γ probe. SLND can proceed quickly with the incision over the skin marking.
Different techniques have been proposed for each step in breast lymphoscintigraphy. Some investigators claim that a radiocolloid containing small particles, such as 99mTc-antimony sulfide colloid (99mTc-ASC; 3–12 nm), allows better migration of tracer and improved detection of sentinel nodes (12), whereas others prefer the larger particles of 99mTc-colloidal albumin (200–1000 nm) because fewer nonsentinel nodes are labeled (9). Often, the agent chosen is the only agent available to the investigator. Currently, no radiopharmaceuticals have been approved for lymphoscintigraphy in the United States. 99mTc-sulfur chloride is approved for intravenous injection and reticuloendothelial imaging but is also widely used for lymphoscintigraphy, both with and without prefiltration (16). 99mTc-human serum albumin, in noncolloidal form, is also approved in the United States for blood-pool imaging, and it has also been widely used as a lymphoscintigraphic agent, although, currently, it is not commercially available. We use sulfur colloid that has been passed through a 0.2-μm filter to select smaller particles; our results compare favorably with those of investigators using other agents (7,9,10,12).
Although we use a peritumoral injection, others such as Veronesi et al. (5) advocate a subdermal injection. In a study comparing subdermal and peritumoral injection techniques, the former reached the sentinel nodes more quickly but no difference was found in the overall sentinel node identification rate (9). Interestingly, most patients received subdermal injections, and overall IM drainage was 2% in this study, much lower than the 11%–39% reported in other series (Table 5). An interesting comparison can be made from a study of cutaneous lymphoscintigraphy patterns obtained for melanoma of the breast skin and anterior trunk on 62 patients using 99mTc-ASC: No IM drainage was recorded (17). Furthermore, Alazraki et al. (18) found that subdermal injections failed to identify IM sentinel nodes that had been revealed by peritumoral injections in the same patients. Therefore, although most breast cancers drain to the axilla, peritumoral injections seem to show somewhat different drainage patterns than subdermal injections.
Injection volume is another variable that is not standardized. Successful sentinel node localization has been achieved using volumes as low as 0.4 mL and as high as 8 mL. Some authors are opposed to larger volumes, believing that such nonphysiologic perturbation may cause erroneous labeling of a lymph node as the sentinel node (17). However, there is no evidence that large injectates will enter lymphatics leading to nonsentinel nodes; rather, greater volumes of injection increase interstitial pressure, which increases lymphatic flow (19). The theoretic merits of a small-volume injection, though conceptually more elegant, have not been proven. Success rates using larger volumes of 99mTc-sulfur chloride are high, the technique is safe, and validation studies with complete axillary dissection have yielded few false-negative sentinel nodes.
CONCLUSION
Breast lymphoscintigraphy with peritumoral injection of 99mTc-sulfur colloid can be performed successfully and is useful before SLND. Sentinel node localization is completed expeditiously and allows demonstration of all regional nodal drainage basins. Most sentinel nodes are located in the axilla, and MOVA, which can be achieved easily with proper patient positioning, enhances detection of AX sentinel nodes during lymphoscintigraphy by obviating overlap of the injection site with the sentinel node. Drainage to IM sentinel nodes cannot be predicted by primary tumor location and requires the anterior view for localization. Larger breast size was associated with longer times for sentinel node localization, but radiopharmaceutical transit time is usually <30 min, which is advantageous for outpatient SLND. We advocate lymphoscintigraphy using anterior and MOVA imaging as an adjunct to the intraoperative γ probe and vital dye for identification of all sentinel nodes in patients with breast cancer.
Acknowledgments
This research was supported in part by funding from the Ben B. and Joyce E. Eisenberg Foundation, Los Angeles, California, and the Fashion Footwear Association of New York.
Footnotes
Received Oct. 19, 1999; revision accepted Feb. 16, 2000.
For correspondence or reprints contact: Edwin C. Glass, MD, Nuclear Medicine Section-115, West Los Angeles VA Medical Center, 11301 Wilshire Blvd., Los Angeles, CA 90073.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Practical Technique to Improve Visualization of Sentinel Nodes in the Axillary Region on Breast Lymphoscintigraphy: Medial Breast Traction by Patient
- Scintigraphic Investigations of the Lymphatic System: The Influence of Injected Volume and Quantity of Labeled Colloidal Tracer
- Usefulness of Medium-Energy Collimator for Sentinel Node Lymphoscintigraphy Imaging in Breast Cancer Patients.
- Continuing Evolution in Breast Cancer Surgical Management
- Reducing Exposure from 57Co Sources During Breast Lymphoscintigraphy by Optimizing Energy Windows and Other Suggested Enhancements of Acquisition and the Display of Images
- Reverse echelon node and a lymphatic ectasia in the same patient during breast lymphoscintigraphy: the importance of injection and imaging technique
- Factors Affecting Visualization Rates of Internal Mammary Sentinel Nodes During Lymphoscintigraphy
- Nonvisualization of Axillary Sentinel Node During Lymphoscintigraphy: Is There a Pathologic Significance in Breast Cancer?