


Abstract
This study investigated the radiographic and scintigraphic courses of union in cervical interbody fusion using hydroxyapatite (HA) grafts or iliac bone autografts. Methods: Twelve patients underwent both serial plain radiography and bone scintigraphy during the 12 mo after surgery. Serial plain radiographs were obtained every month until the end of the study period. Bone scintigrams with 99mTc-hydroxymethylene diphosphonate (HMDP) were obtained at 2 wk and at 1, 2, 3, and 6 mo. Uptake of 99mTc-HMDP in the graft was expressed as a ratio of the counts in the graft to those in the axis. Results: In the HA graft group, the plain radiographs of all patients showed a radiolucent stripe that disappeared 7.3 ± 1.5 (mean ± SD) months after surgery. In the autograft group, a radiolucent stripe around the graft was not seen for any patient, and union was confirmed by follow-up radiographs within 6 mo after surgery. The serial changes in the 99mTc-HMDP uptake ratio showed no difference between the 2 groups. The 99mTc-HMDP uptake ratio peaked 1 mo after surgery and decreased rapidly to a plateau within 2 mo. Conclusion: In the HA graft group, despite the presence of a radiolucent stripe around the graft for more than 6 mo, the scintigraphic course of union was not different from that in the autograft group. The likelihood is that the presence of a radiolucent stripe around the HA graft in the early months after surgery is not always a sign of pseudoarthrosis.
Recently, synthetic hydroxyapatite (HA) has been used as a substrate in cervical interbody fusion (1–4). Unlike autogeneic or allogeneic bone grafts, HA undergoes little absorption and becomes surrounded by autologous bridging bone, which eventually fuses with adjacent vertebrae. Direct bonding of HA grafts with the adjacent bone has also been confirmed by electron microscopy (2,5). Although this bonding has been reported to occur within a short (6- to 8-wk) period (1), plain radiographs after HA grafting often reveal a radiolucent stripe along the surface of the HA graft for more than 6 mo. This stripe is a radiographic feature of pseudoarthrosis or failure of union in patients with autologous or allogeneic grafting (6,7). The purpose of our study was to clarify the course of union of HA grafts with adjacent vertebrae using serial plain radiographs and 99mTc-hydroxymethylene diphosphonate (HMDP) bone scintigrams.
MATERIALS AND METHODS
Patient Population
Between March 1997 and February 1998, 12 patients underwent cervical interbody fusion: 6 patients with HA grafts and 6 patients with iliac bone autografts. Anterior interbody fusion was performed on patients with symptomatic pathology of the ventral root of the cervical spine or compression of the cord. Single interbody fusion was performed on all patients. All 12 patients were prospectively evaluated with serial anteroposterior and lateral radiographs and bone scintigraphy. The patients were randomly assigned to either the HA graft or the autograft group before surgery.
Operation and Grafting Materials
In patients with HA grafting, the superior and inferior vertebral cortical end plates were removed with an air drill after diskectomy to expose the cancellous part of the vertebral bodies. After preparation of the bone cavity to accommodate the HA graft, the osteophytes and other offending structures were resected and the HA graft was inserted. The HA ceramic graft was 40% porous and shaped like a lens, as designed by Kim et al. (4). In patients with autologous bone grafting, the operations were performed similarly except that vertebral body end plates were partially decorticated, without exposure of cancellous bone. The iliac bone autograft was harvested from the patient's anterior iliac crest. All patients wore a Philadelphia cervical collar for 2 mo postoperatively.
Imaging Studies
Serial anteroposterior and lateral plain radiographs were obtained every month postoperatively. Lateral flexion–extension views were obtained at 2 mo. Plain radiographs were obtained as analog images. The postoperative radiographs were read separately by 2 observers to evaluate the presence or absence of a radiolucent stripe along the surface of the graft. Then, the 2 observers reached a consensus about those studies for which the individual readings differed.
Postoperative bone scintigrams were sequentially obtained at 2 wk and at 1, 2, 3, and 6 mo. Bone scintigrams were obtained 4 h after an intravenous infusion of 740 MBq 99mTc-HMDP. Anteroposterior and lateral cervical images were obtained using a gamma camera (Optima; GE-YMS, Tokyo, Japan) equipped with a low-energy, parallel-hole, high-resolution collimator. A 256 × 256 digital image was obtained in a preset time of 5 min. The regions of interest were placed on the center of the graft, and the axis was placed in the lateral view (10.5 × 10.5 mm). The uptake of 99mTc-HMDP in the graft was expressed as a ratio of the counts in the graft to those in the axis. Counts were read 3 times in the graft and axis, and the average of the readings was used. The association between scintigraphic characteristics and fusion substrates was tested by repeated ANOVA with commercially available software (StatView 4.5 J; Abacus Concepts, Berkeley, CA).
RESULTS
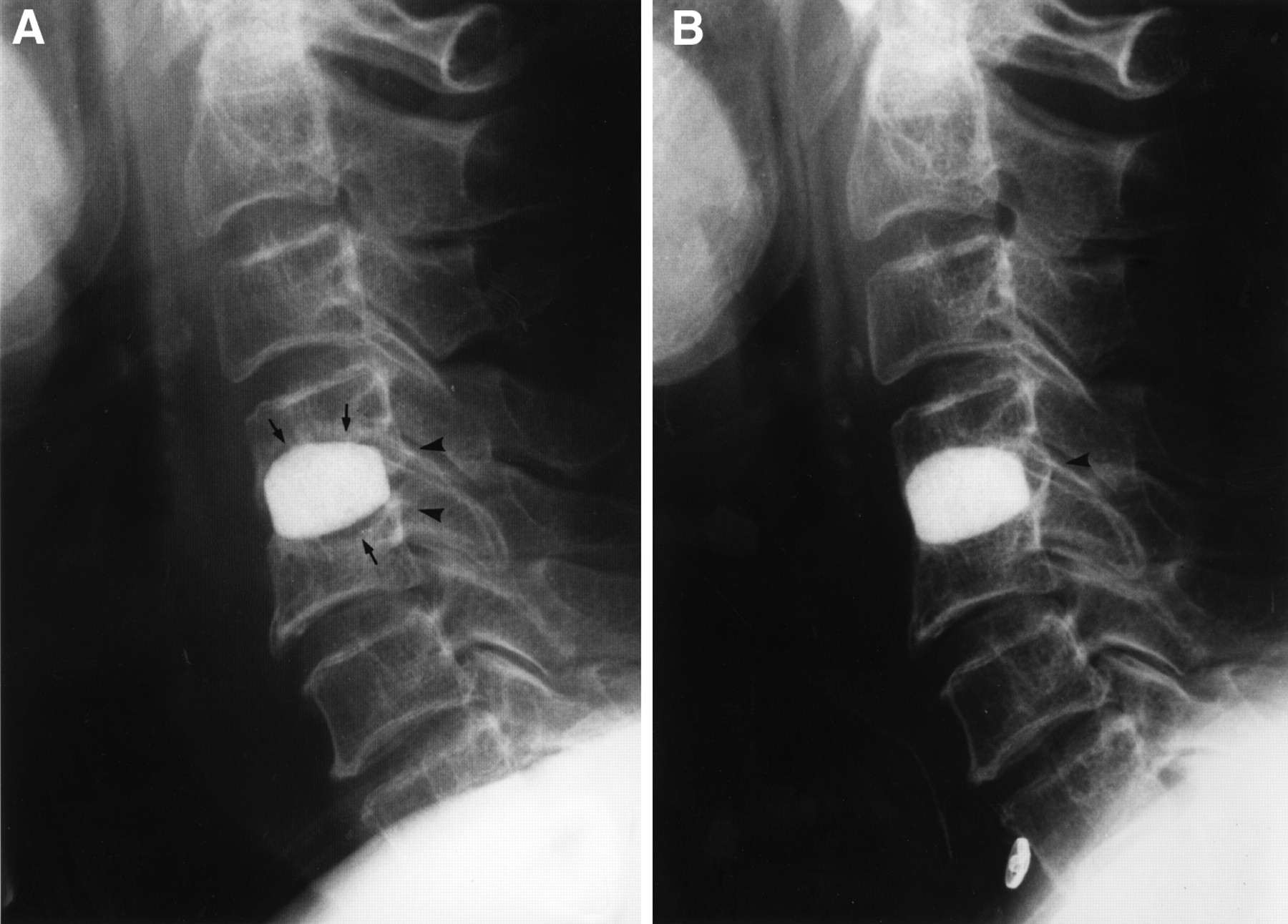
In all patients, stability of the graft was confirmed by dynamic radiographs 2 mo after surgery. Neurologic deterioration related to the fusion segment was not observed in any patient. The clinical and radiologic characteristics of each group are shown in Table 1. In all patients of the HA graft group, plain radiographs showed a radiolucent stripe that disappeared between 6 and 10 mo after surgery (mean ± SD, 7.3 ± 1.5 mo) (Fig. 1). Formation of bridging bone on the surface of the grafts became evident between 3 and 6 mo after surgery. Neither dislocation and breakage of the HA grafts nor collapse of the adjacent vertebral bodies was observed. In no patient of the autograft group was a radiolucent stripe seen around the graft. Complete bridging of trabeculae between the bone graft and the adjacent vertebral bodies was observed within 6 mo after surgery (Fig. 2).
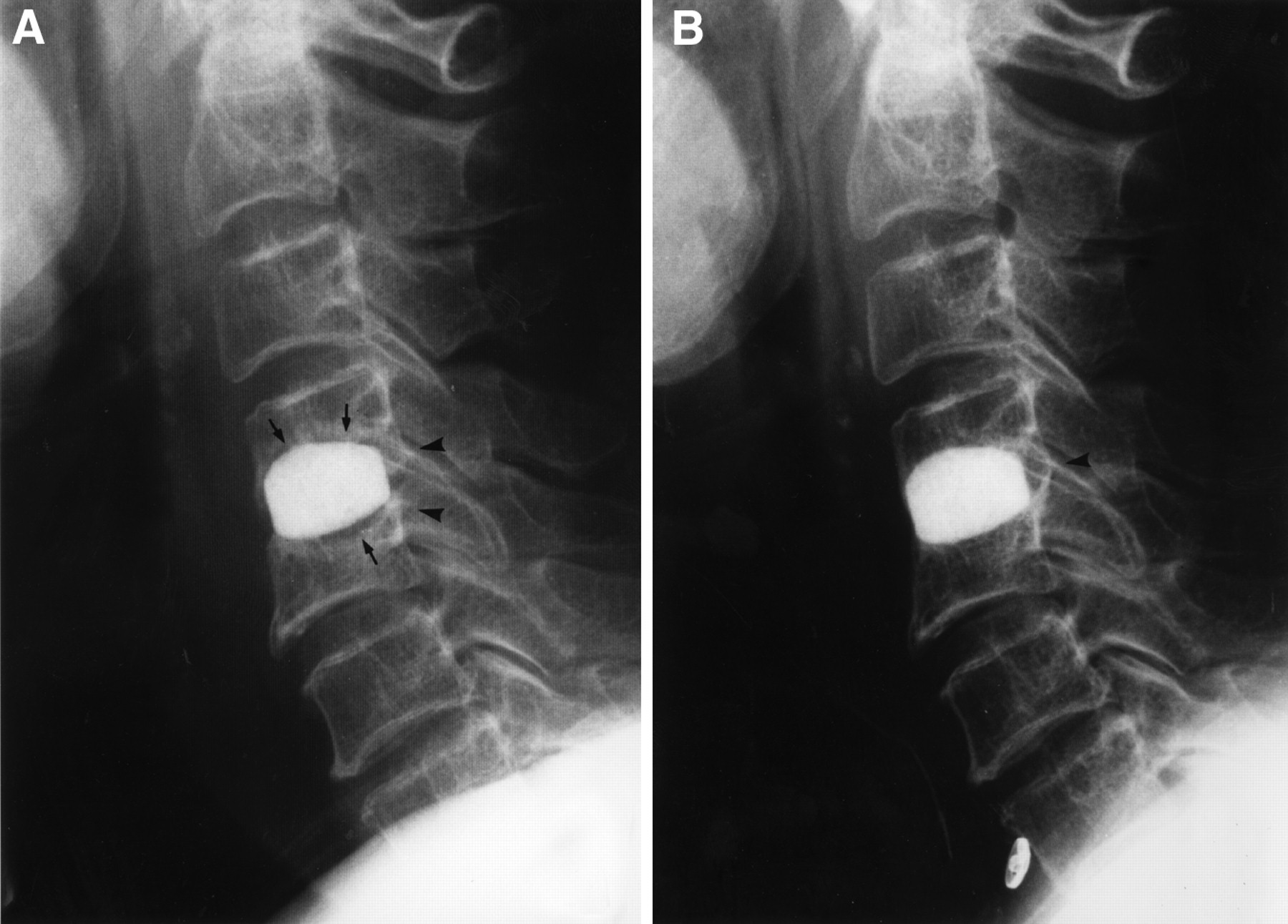
Plain radiographs of 66-y-old woman after C4–C5 fusion using HA graft. (A) Postoperative lateral radiograph at 3 mo shows apparent radiolucent stripe (arrows) around graft and bone growth adjacent to vertebral bodies (arrowheads). (B) Postoperative lateral radiograph at 10 mo shows bridging bone (arrowhead) at dorsal aspect of graft and disappearance of radiolucent stripe.

Plain radiograph of 60-y-old man after C5–C6 fusion using autograft. Postoperative lateral radiograph at 5 mo shows complete bridging of trabeculae between graft and adjacent vertebral bodies.
Clinical and Radiologic Characteristics
Figure 3 shows serial changes in the 99mTc-HMDP uptake ratio for HA grafts and autografts during the fusing period. The 99mTc-HMDP uptake ratio peaked 1 mo after surgery (2.33 ± 0.20 in the HA graft group and 2.15 ± 0.07 in the autograft group) and decreased rapidly to a plateau level of 1.6 within 2 mo in both groups. Thereafter, in both groups, a 99mTc-HMDP uptake ratio of 1.6 lasted until the end of the study. 99mTc-HMDP uptake ratios for 2 groups were analyzed by repeated-measures ANOVA. No significant difference in serial changes in the 99mTc-HMDP uptake ratio were seen between the 2 groups (F4 = 1.452, P = 0.235).

Serial changes in 99mTc-HMDP uptake ratio for HA grafts (○) and iliac bone autografts (□).
DISCUSSION
Our study showed that serial changes in the 99mTc-HMDP uptake ratio for HA grafts during the fusing period were not different from those for autografts. The 99mTc-HMDP uptake ratio peaked 1 mo after surgery and decreased rapidly to a plateau within 2 mo. Thereafter, a low uptake ratio of 1.6 remained until the end of the study. These serial scintigraphic findings are in accordance with those found in studies of normal healing of femoral neck (8) and distal radius (9) fractures. In those studies, however, the peak uptake ratio of the fracture lesion to the contralateral normal region reached as much as 3:12. Compared with these studies, the lower peak in our study may have been caused by measurement of tracer uptake in the grafts isolated from vascular supply (10).
Judging from the serial changes in the 99mTc-HMDP uptake ratio for HA grafts, we suggest that the active growth of bone around the grafts occurs within 2 mo after surgery. These results are in accordance with the results of a histologic study reported by Akino (11). In his experimental study, in which HA grafts with 30% porosity were implanted in canine cervical vertebrae, bone growth into the pores and on the surface of the grafts was observed 1 mo after surgery. The amount of bone formation increased for up to 2 mo and then became stable.
With plain radiography, a radiolucent stripe along the surface of all HA grafts was observed for more than 6 mo. This stripe is a radiographic feature of pseudoarthrosis or failure of union in cases of autologous or allogeneic grafting (6,7). The radiographic time course of a radiolucent stripe around the HA graft in this study is consistent with that in previous reports (12,13). In a study using HA to replenish a bone defect after harvesting an iliac bone graft or resecting a benign bone tumor, a radiolucent stripe around the HA graft was routinely observed and disappeared during an average of 10 mo after surgery (13).
CONCLUSION
From these considerations, it is likely that a radiolucent stripe around the HA graft in cervical interbody fusion in the early months after surgery is not always a sign of pseudoarthrosis.
Footnotes
Received Aug. 25, 1999; revision accepted May 16, 2000.
For correspondence or reprints contact: Tsutomu Iseda, MD, Department of Neurosurgery, Miyazaki Medical College, 5200, Kihara, Kiyotake, Miyazaki 889-1692, Japan.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.